Bulletin N° 1010
“The
Last Mission”
[of Dag Hammarskjold]
https://www.youtube.com/watch?v=_M8iBVk71Zk
(1:14:58)
This 1976 documentary, directed by Tristram Powell is a powerful portrayal of moral idealism gone off the rails, with references to Conor Cruise O'Brien’s play, “Murderous Angels.” It depicts the spiritual aspects of the post genocide policies in the Congo, after Belgium troops were forced to leave and western diplomacy took over.
Dag
Hammarskjöld, born July 29, 1905, Jönköping, Sweden—died September 18, 1961,
near Ndola, Northern Rhodesia [now Zambia]), Swedish economist and statesman
who, as the second secretary-general (1953–61) of the United Nations (UN),
enhanced the prestige and effectiveness of that organization. He was
posthumously awarded the Nobel Prize for Peace in 1961.
Subject: Post-Humanist cynics fulfilling
our destiny: Dr. Fauci and Mother Teresa standing guard by the toilet flush,
watching the inevitable occur at the leaking sewer pipes. (FACT CHECK: USA TODAY)
Grenoble, November 21,
2021
Dear Colleagues and Friends of
CEIMSA,
As participants in
this correspondence community at the CEIMSA research center, you are familiar
with the principle objectives we have pursued over the past many years, namely to provide students and colleagues with information about currents events which is circulating in
the Anglophone world. As I am a social historian by training,
with a Ph.D. from the University of Wisconsin, I have
presented in these bulletins many books written by historians who in my opinion have made significant contributions to our understanding of history and our contemporary
society. I have no interest in dictating the TRUTH to others, as I have become
convinced over the years that truth is a pursuit, and not a destination, and
without a wide range of information and points of view there is no possibility
of making progress in this endeavor. In the absence of this pursuit, we risk being
paralyzed by the injunctions of Dictators –either the so-called “left” or “right” –
who historically have easily morphed into Executioners.
It should be abundantly clear that I
make no claims to any expertise in the fields of natural science and medicine.
The views presented in the articles and essays I have shared in CEIMSA bulletins represent information and
discussions that I think must be evaluated openly and publically by all parties
concerned. It is precisely through public discussions (the anathema to
censorship) that the pursuit of truth is accomplished, and that charlatans and
criminals are exposed. The wisdom gained from unimpeded public discussion is reflected
in Alfred North Whitehead’s book, Modes of Thought (1958), where he writes: “Thus
beyond all questions of quantity, there lie questions of pattern, which are
essential for the understanding of nature. Apart from a presupposed pattern,
quantity determines nothing.”
It goes almost
without saying that any medical advice should be sought from qualified medical
experts whom you trust to be well-informed and sincerely concerned with your well being.
At best some of the information provided in these selected articles and essays
have the heuristic value of raising questions that might be of assistance in
private consultations with family physicians to arrive at an authentic
experience of “informed consent”.
On the other hand, the professional ethics of the historian present their own demands, which are discussed in the conclusion of Barrington Moore, Jr.’s 1966 book, Social Origins of Dictatorship and Democracy: Lord and Peasant in the Making of the Modern World.
There is a respectable intellectual tradition which denies that objectivity is possible at all, even in principle. This denial seems to rest on confusion between the causes of historical events and their consequences or meaning. The causes of the American Civil War had run their course by the time the first shot was fired at Fort Sumter. No historian’s opinion about these causes can have the remotest effect on what they actually were. The consequences are another matter. They are with us today and may be with us as long as human history continues. This second aspect of the thesis about the permanent ambiguity of history seems to be perfectly valid. Statements by historians about the causes of the Civil War have polemical results now, no matter what their authors intend. It is in this sense that impartiality is an impossibility and an illusion. Whether he knows it or not, to continue the argument the historian has to adopt some principle in selecting and ordering his facts. The same is true for the sociologist studying contemporary affairs. By virtue of what they include and exclude, highlight or deemphasize, these principles have political and moral consequences. Hence they are unavoidably moral principles. It is impossible to opt out of the struggle. The very act of trying to opt out, of trying to take a nonpartisan position, means taking up a form of apolitical pseudo-objectivity that in effect supports the status quo.
The thesis that neutrality is impossible is a powerful one, convincing at any rate to me. But I do not think that it leads to a denial that objective social and historical analysis is possible. Different perspectives on the same set of events should lead to complementary and congruent interpretations, not to contradictory ones. Furthermore the denial that objective truth is possible in principle flings open the door to the worst forms of intellectual dishonesty. A crude version goes something like this: since neutrality is impossible I will take my stand with the underdog and write history to serve the underdog, helping in this way to reach a ‘higher Truth.’ In plain language that is just cheating No matter what his unavoidable moral premises and predilections, any student of human affairs is bound sooner or later to come across evidence that is profoundly disturbing. Then he has the task of coming to terms with it honestly.
Gradations of Truth with a capital T, rightly in my estimation, arouse angry suspicion. But this does not mean that objectivity and truth with a small t lead to comfortable complacency. Objectivity is not the same thing as conventional judiciousness. A celebration of the virtues of our own society which leaves out its ugly and cruel features, which fails to face the question of a connection between its attractive and its cruel ones, remains an apologia even if it is spoken in the most measured academic tones. There is a strong tendency to assume that mild-mannered statements in favor of the status quo are ‘objective’ and that anything else is a form of ‘rhetoric.’
This type of bias, this misinterpretation of objectivity, is the one most common in the West today. It confuses objectivity with triviality and meaninglessness. For reasons already mentioned, any simple straightforward truth about political institutions or events is bound to have polemical consequences. It will damage some group interests. In any society the dominant groups are the ones with the most to hide about the way society works. Very often therefore truthful analyses are bound to have a critical ring, to seem like exposures rather than objective statements, as the term is conventionally used. (This will be true in communist counties too if they ever get to the point of allowing moderately candid accounts of their own past to see the light.) For all students of human society, sympathy with the victims of historical processes and skepticism about the victors’ claims provide essential safeguards against being taken in by the dominant mythology. A scholar who tries to be objective needs these feelings as part of his ordinary working equipment.(pp.521-523)
These warning from
the past server as a contradistinction to our actual intellectual state of mind
in the creeping totalitarianism we are witnessing today, where shameless
collaboration is the new normal, and existential fear is the staple diet for the
mass manufactured cowards who cling relentlessly to the hem of the Grand
Inquisitor’s gown in a desperate search for security.
Sincerely,
Francis McCollum Feeley
--
Professeur
honoraire de l'Université Grenoble-Alpes
Ancien Directeur des Researches
Université de Paris-Nanterre
Director of The Center for the Advanced Study
of American Institutions and Social Movements
(CEIMSA-in-Exile)
The University of California-San Diego
http://www.ceimsa.org
a.
“Gaze Into the Orb to Collect Your
Worldcoin”
https://www.corbettreport.com/nwnw20211118/
with James Corbett and James Even Pilato
(29:02)
+
Revealed: Documents Show Bill Gates Has Given $319 Million to
Media Outlets
by Alan
MacLeod
+
Bill Gates Caught Buying Positive News Coverage
https://www.youtube.com/watch?v=GcCQVkpWMcE
with Jimmy Dore and Max Blumenthal
(1:00:59)
+
Vaccinated English adults under 60 are dying at twice the rate of unvaccinated people the same age and have been for six months
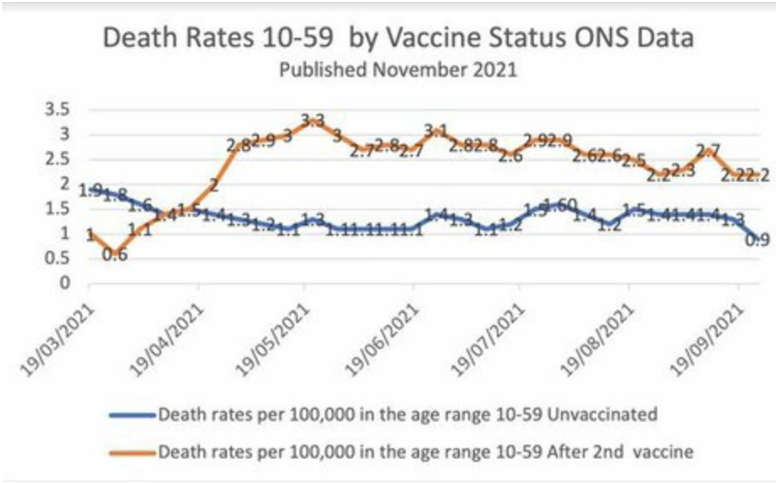
This chart may seem unbelievable or impossible, but it's correct, based on weekly data from the British government.
+
Denis Rancourt Interview - How A Deep Dive Analysis Of COVID Data
Reveals A Pandemic
Did Not Occur
with Ryan
Cristián and Denis Rancourt
(1:36:57)
+
‘Fauci's
Greatest Covid Failures’ Exposed
with Jimmy
Dore
(20:20)
+
Rand
Paul Warns ‘Authoritarian’
Fauci's ‘Casual Disdain’ For Rights Is ‘Recipe For
Totalitarianism’
by Steve Watson via Summit News,
Appearing on Fox News Wednesday, Senator Rand Paul
continued his long running exposition of Anthony Fauci, warning viewers that
Fauci’s latest comments provide yet anoher example of how brazenly
“authoritarian” he is.
+
Interview
1675 - The REAL Anthony Fauci with Robert F. Kennedy, Jr.
https://www.corbettreport.com/fauci/?utm_source=feedburner&utm_medium=email
with James Corbett
and Robert Kennedy
(1:03:12)
+
The Covid Outbreak: ‘Biggest Health Scam of the 21st Century’
Report
by 1500 Health Professionals
by United
Health Professionals
===========
b.
If You Take the COVID Vax, You Can Never Achieve Full Immunity Again
– Government Stats
Unveil the Horrifying Truth
by Ethan
Huff
+
Everyone Missed this One... Vaccinated People Are Up to Nine Times (9X)
More Likely to
be Hospitalized than Unvaccinated People
by Steve
Kirsch
+
Trends in Mortality and Morbidity in the Most Vaccinated Countries :
Twenty-one Proven Facts

by Gérard
Delépine
+
FDA
report finds all-cause mortality higher among vaccinated
https://www.israelnationalnews.com/News/News.aspx/317091
by David
Rosenberg
+
Worldwide
Search Trend for "Died Suddenly" Spikes to Record Highs
https://www.globalresearch.ca/worldwide-search-trend-died-suddenly-spikes-record-highs/5762053
by Zero Hedge
+
Vaccine
Damage Payouts In UK Could Soar Next Year
https://www.zerohedge.com/covid-19/vaccine-damage-payouts-uk-could-soar-next-year
by Owen Evans via The Epoch Times,
The number of claims
for the UK’s vaccine injury scheme is expected to be 18
times higher next year, according to a
government-backed health body.
===========
c.
Derrick Broze Interview - The Great Narrative And The Metaverse: Your
Coming Dystopian
Future

with
(51:55)
+
This
Week's Most Popular Articles
https://www.globalresearch.ca/this-weeks-most-popular-articles-49/5762116
+
America’s Largest Teachers’ Unions Push Vaccine Mandates That Will
Usher in Technocratic
Digital ID
by John
Klyczek
+
California City Designates Itself ‘Sanctuary City’
Against COVID Mandates

by Leslie
Eastman
+
OSHA Suspends Biden’s Employer Vaccine Mandates
Following Court Order
+
Homicide Rates In 2020 Surged To 24-Year High...
Another
Sign Of A Failing Regime
by Ryan McMaken via The Mises Institute
+
‘These Are Numbers We Have Never Seen Before’:
Drug
Overdose Deaths Hit Record High During Pandemic

by Tyler
Durden
As the pandemic swept across the country, a record number
of Americans died of drug overdoses
in the 12-month period ending in April 2021, according to preliminary
data released by the
Centers for Disease Control and Prevention (CDC). The more than 100,000 overdose deaths is nearly 30% higher than the 78,000 counted the
year before - with much of the blame landing on the availability and potency of
synthetic opioids such as Fentanyl - which is up to 50x more potent than
heroin, according to Statista, which notes that
the CDC has reported more than 60% of
overdose deaths last year involved synthetic opioids
+
US drug overdose deaths top 100,000 in
one year in 28.5% increase
https://www.aljazeera.com/news/2021/11/17/us-drug-overdose-deaths-top-100000-in-one-year
by Aljazeera
===========
d.
The Road To Fascism:
Paved With Vaccine Mandates And
Corporate Collusion
https://www.zerohedge.com/political/road-fascism-paved-vaccine-mandates-and-corporate-collusion
by John W.
Whitehead & Nisha Whitehead via The
Rutherford Institute
+
Vaccine Injury Attorney Suing the FDA: FDA Asks Federal Judge to
Grant it Until the Year 2076 to Fully Release Pfizer’s COVID-19
Vaccine Data
by Brian
Shilhavy
+
FDA Wants Until 2076 To Fully Release Pfizer Vaccine Data: Lawsuit

https://www.zerohedge.com/covid-19/fda-wants-until-2076-fully-release-pfizer-vaccine-data-lawsuitby
by Attorney Aaron Siri via Injecting Freedom
+
More People Died in the Key Clinical Trial for Pfizer's COVID
Vaccine
than
the Company Publicly Reported
by Alex Berenson
+
FDA asks for 55 years to release data on Pfizer's COVID vaccine

https://www.israelnationalnews.com/News/News.aspx/317161
by Y
Rabinovitz
+
COVID-19: Moderna Gets Its Miracle
https://unlimitedhangout.com/2021/10/investigative-reports/covid-19-moderna-gets-its-miracle/
analysis by
Whitney Webb
(1:23:45)
Story
at-a-glance
- Moderna
and a handful of its collaborators at the National Institutes of Health
(NIH) seemed to know that Moderna’s miracle had arrived — well before
anyone else knew or could have known
- Moderna’s
CEO Stéphane Bancel emailed the director of the NIH and asked to be sent
the genetic sequence for what would become known as SAR-CoV-2, allegedly
because media reports on the outbreak “troubled” him
- In
order to begin its human trial, regulatory agencies had to allow Moderna
to bypass major aspects of traditional animal trials, which many experts
and commentators noted was highly unusual but was now deemed necessary due
to the urgency of the crisis
- Instead
of developing the vaccine in distinct sequential stages, as is the custom,
Moderna “decided to do all of the steps [relating to animal trials]
simultaneously”
- US
taxpayers may have an ownership stake in vaccines made and sold by Moderna
COVID-19 erased the regulatory and trial-related hurdles
that Moderna could never surmount before. Yet, how did Moderna know that
COVID-19 would create those conditions months before anyone else, and why did
they later claim that their vaccine being tested in NIH trials was different
than their commercial candidate?
In late 2019, the biopharmaceutical company Moderna was
facing a series of challenges that not only threatened its ability to ever take
a product to market, and thus turn a profit, but its very existence as a
company.
There were multiple warning signs that Moderna was
essentially another Theranos-style fraud, with many of these signs growing in
frequency and severity as the decade drew to a close. Part
I
of this three-part series explored the disastrous circumstances in which
Moderna found itself at that time, with the company's salvation hinging on the
hope of a divine miracle, a "Hail Mary" save of sorts, as stated by
one former Moderna employee.
While the COVID-19 crisis that emerged in the first part of
2020 can hardly be described as an act of benevolent divine intervention for
most, it certainly can be seen that way from Moderna's perspective. Key issues
for the company, including seemingly insurmountable regulatory hurdles and its
inability to advance beyond animal trials with its most promising — and
profitable — products, were conveniently wiped away, and not a moment too soon.
Since January 2020, the value of Moderna's stock — which had
embarked on a steady decline since its IPO — grew from $18.89 per share to its
current value of $339.57 per share, thanks to the success of its COVID-19
vaccine.
Yet, how exactly was Moderna's "Hail Mary" moment
realized, and what were the forces and events that ensured it would make it
through the FDA's emergency use authorization (EUA) process? In examining that
question, it becomes quickly apparent that Moderna's journey of saving grace
involved much more than just cutting corners in animal and human trials and
federal regulations.
Indeed, if we are to believe Moderna executives, it involved
supplying formulations for some trial studies that were not the same as their
COVID-19 vaccine commercial candidate, despite the data resulting from the
former being used to sell Moderna's vaccine to the public and federal health
authorities.
Such data was also selectively released at times to align
with preplanned stock trades by Moderna executives, turning many of Moderna's
highest-ranking employees into millionaires, and even billionaires, while the
COVID-19 crisis meant economic calamity for most Americans.
Not only that, but — as Part II of this three-part series
will show, Moderna and a handful of its collaborators at the National
Institutes of Health (NIH) seemed to know that Moderna's miracle had arrived —
well before anyone else knew or could have known.
Was it really a coincidental mix of "foresight"
and "serendipity" that led Moderna and the NIH to plan to develop a
COVID-19 vaccine days before the viral sequence was even published and months
before a vaccine was even considered necessary for a still unknown disease? If
so, why would Moderna — a company clearly on the brink — throw everything into
and gamble the entire company on a vaccine project that had no demonstrated
need at the time?
The
Serendipitous Origins of Moderna's COVID-19 Vaccine
When early January 2020 brought news of a novel coronavirus
outbreak originating in Wuhan, China, Moderna's CEO Stéphane Bancel immediately
emailed Barney Graham, deputy director of the Vaccine Research Center at the
National Institutes of Health, and asked to be sent the genetic sequence for
what would become known as SAR-CoV-2, allegedly because media reports on the
outbreak "troubled" him.
The date of that email varies according to different media
reports, though most place it as having been sent on either January 6th or 7th.
A few weeks before Bancel's email to Graham, Moderna was quickly approaching
the end of the line, their desperately needed "Hail
Mary"
still not having materialized.
"We were freaked out about money," Stephen Hoge
would later remember of Moderna's late 2019 circumstances.
Not only were executives "cutting back on research and
other expenditures" like never before, but – as STAT
News
would later report – "cash from investors had stopped pouring in and
partnerships with some drug makers had been discontinued. In meetings at
Moderna, Bancel emphasized the need to stretch every dollar and employees were
told to reduce travel and other expenses, a frugality there were advised would
last several years."
At the tail end of 2019, Graham was in a very different mood
than Bancel, having
emailed
the leader of the coronavirus team at his NIH lab saying, "Get ready for
2020," apparently viewing the news out of Wuhan in late 2019 as a
harbinger of something significant.
He went on, in the days before he was contacted by Bancel,
to "run a drill he had been turning over in his mind for years" and
called his long-time colleague Jason McLellan "to talk about the game
plan" for getting a head start on producing a vaccine the world did not
yet know it needed.
When Bancel called Graham soon afterward and asked about
this new virus, Graham responded that he didn't know yet but that "they
were ready if it turned out to be a coronavirus." The
Washington Post claimed that Graham's apparent foreknowledge that a
coronavirus vaccine would be needed before anyone officially knew what type of
disease was circulating in Wuhan was a fortunate mix of "serendipity and
foresight."

Dr. Barney Graham and Dr. Kizzmekia Corbett, VRC coronavirus
vaccine lead, discuss COVID-19 research with U.S. legislators Sen. Chris Van Hollen,
Sen. Benjamin Cardin and Rep. Jamie Raskin, March 6, 2020; Source: NIH
A report in Boston
magazine
offers a slightly different account than that reported by the Washington Post.
Per that article, Graham had told Bancel, "If [the virus] is a
coronavirus, we know what to do and have proven mRNA is effective."
Per that report, this assertion of efficacy from Graham
referred to Moderna's early
stage human-trial data published in September 2019 regarding its chikungunya
vaccine candidate, which was funded by the Defense Advanced Research Projects
Agency (DARPA), as well as its cytomegalovirus (CMV) vaccine candidate.
As mentioned in Part
I
of this series, the chikungunya vaccine study data released at that time
included the participation of just four subjects, three of whom developed
significant side effects that led Moderna to state that they would reformulate
the vaccine in question and would pause trials on that vaccine candidate.
In the case of the CMV vaccine candidate, the data was
largely positive, but it was widely noted that the vaccine still needed to pass
through larger and longer clinical trials before its efficacy was in fact
"proven," as Graham later claimed.
In addition, Graham implied that this early stage trial of
Moderna's CMV vaccine candidate was somehow proof that an mRNA vaccine would be
effective against coronaviruses, which makes little sense since CMV is not a
coronavirus but instead hails from the family of viruses that includes
chickenpox, herpes, and shingles.
Bancel apparently had reached out to Graham because Graham
and his team at the NIH had been working in direct partnership with Moderna on
vaccines since 2017, soon after Moderna had delayed its Crigler-Najjar and
related therapies in favor of vaccines.
According to Boston
magazine,
Moderna had been working closely with Graham specifically "on [Moderna's]
quest to bring a whole new class of vaccines to market" and Graham had personally
visited
Moderna's facilities in November 2019. Dr. Anthony Fauci, the director of the
NIH's infectious-disease division NIAID, has called his unit's collaboration
with Moderna, in the years prior to and also during the COVID-19 crisis, "most
extraordinary."
The year 2017, besides being the year when Moderna made its
pivot to vaccines (due to its inability to produce safe multidose therapies,
see Part
I),
was also a big year for Graham.
That year he and his lab filed
a patent
for the "2P mutation" technique whereby recombinant coronavirus spike
proteins can be stabilized in a prefusion state and used as more effective
immunogens. If a coronavirus vaccine were to be produced using this patent,
Graham's team would financially benefit, though federal law caps their annual
royalties. Nonetheless, it would still yield a considerable sum for the named
researchers, including Graham.
However, due to the well-known difficulties with coronavirus
vaccine development, including antibody dependent enhancement risk, it seemed
that commercial use of Graham's patent was a pipe dream. Yet, today, the
2P mutation patent, also known as the '070 patent, is not just in use in
Moderna's COVID-19 vaccine, but also in the COVID-19 vaccines produced by
Johnson & Johnson, Novavax, Pfizer/BioNTech, and CureVac.
Experts at New York University School of Law have
noted
that the 2P mutation patent first filed in 2016 "sounds remarkably
prescient" in light of the COVID crisis that emerged a few years later
while later publications from the NIH (still pre-COVID) revealed that the NIH's
view on "the breadth and importance of the '070 patent" as well as
its potential commercial applications was also quite prescient, given that
there was little justification at the time to hold such a view.
On January 10, three days after the reported initial
conversation between Bancel and Graham on the novel coronavirus outbreak in
Wuhan, China, Graham met with Hamilton Bennett, the program leader for
Moderna's vaccine portfolio.
Graham asked Bennett "if Moderna would be interested in
using the new [novel coronavirus] to test the company's accelerated
vaccine-making capabilities." According to Boston, Graham
then mused, "That way ... if ever there came a day when a new virus emerged
that threatened global public health, Moderna and the NIH could know how long
it would take them to respond."
Graham's "musings" to Bennett are interesting
considering his earlier statements made to others, such as "Get ready for
2020" and his team, in collaboration with Moderna, would be "ready if
[the virus then circulating in Wuhan, China] turned out to be a
coronavirus." Is this merely "serendipity" and
"foresight", as the Washington Post suggested, or was it something
else?
It is worth noting that the above accounts are those that
have been given by Bancel and Graham themselves, as the actual contents of
these critical January 2020 emails have not been publicly released.
When the genetic sequence of SARS-CoV-2 was published on
January 11, NIH scientists and Moderna researchers got to work determining
which targeted genetic sequence would be used in their vaccine candidate. Later
reports, however, claimed that this initial work toward a COVID-19 vaccine was
merely intended to be a "demonstration
project."
Other odd features of the Moderna-NIH COVID-19
vaccine-development story emerged with Bancel's
account
of the role the World Economic Forum played in shaping his
"foresight" when it came to the development of a COVID-19 vaccine
back in January 2020.
On January 21, 2020, Bancel reportedly
began to hear about "a far darker version of the future" at the
World Economic Forum (WEF) annual meeting in Davos, Switzerland, where he spent
time with "two [anonymous] prominent infectious-disease experts from
Europe" who shared with him data from "their contacts on the ground
in China, including Wuhan."
That data, per Bancel, showed a dire situation that left his
mind "reeling" and led him to conclude, that very day, that
"this isn't going to be SARS. It's going to be the 1918 flu
pandemic."

Stéphane Bancel speaks at the Breakthroughs in Cancer Care
session at WEF annual meeting, January 24, 2020; Source: WEF
This realization is allegedly what led Bancel to
contact
Moderna cofounder and chairman, as well as a WEF
technology pioneer, Noubar Afeyan. Bancel reportedly interrupted Afeyan's
celebration of his daughter's birthday to tell him "what he'd learned
about the virus" and to suggest that "Moderna begin to build the
vaccine — for real."
The next day, Moderna held an executive meeting, which
Bancel attended remotely, and there was considerable internal debate about
whether a vaccine for the novel coronavirus would be needed.
To Bancel, the "sheer act of debating" pursuing a
vaccine for the virus was "absurd" given that he was now convinced,
after a single day at Davos, that "a global pandemic was about to descend
like a biblical plague, and whatever distractions the vaccine caused internally
at Moderna were irrelevant."
Bancel spent the rest of his time at the Davos annual
meeting "building partnerships, generating excitement, and securing
funding," which led to the Moderna collaboration agreement with the
Coalition for Epidemic Preparedness Innovations — a project largely funded by
Bill Gates.
(Bancel and Moderna's cozy relationship with the WEF, dating
back to 2013, was discussed in Part
I
as were the Forum's efforts, beginning well before COVID-19, to promote
mRNA-based therapies as
essential
to the remaking of the health-care sector in the age of the so-called Fourth
Industrial Revolution).
At the 2020 annual meeting attended by Bancel and others it
was noted that a major barrier to the widespread adoption of these and other
related "health-care" technologies was "public distrust."
The panel where that issue was specifically discussed was entitled "When
Humankind Overrides Evolution."
As also noted in Part
I
of this series, a few months earlier, in October 2019, major players in what
would become the Moderna COVID-19 vaccine, particularly Rick Bright and Anthony
Fauci, had discussed during a Milken Institute panel on vaccines how a
"disruptive" event would be needed to push the public to accept
"nontraditional" vaccines such as mRNA vaccines; to convince the
public that flu-like illnesses are scarier than traditionally believed; and to
remove existing bureaucratic safeguards in the vaccine development-and-approval
processes.
That panel took place less than two weeks after the Event
201 simulation, jointly hosted by the World Economic Forum, the Bill &
Melinda Gates Foundation, and the Johns Hopkins Center for Health Security.
Event 201 simulated "an
outbreak of a novel zoonotic coronavirus" that was "modeled largely
on SARS but ... more transmissible in the community setting by people with mild
symptoms." The recommendations of the
simulation panel were to considerably increase investment in new vaccine
technologies and industrial approaches, favoring rapid vaccine development and
manufacturing.
As mentioned in Part
I,
the Johns Hopkins Center for Health Security had also conducted the June 2001
Dark Winter simulation that briefly preceded and predicted major aspects of the
2001 anthrax attacks, and some of its participants had apparent foreknowledge
of those attacks. Other Dark Winter participants later worked to sabotage the
FBI investigation into those attacks after their origin was traced back to a US
military source.
It is hard to imagine that Bancel, whose company had long
been closely partnered with the World Economic Forum and the Gates Foundation,
was unaware of the exercise and surprised by the closely analogous event that
transpired within three months.
Given the accounts given by Bancel, Graham, and others, it
seems likely there is more to the story regarding the origins of Moderna's
early and "serendipitous" push to develop a COVID-19 vaccine.
In addition, given that Moderna was in dire financial
circumstances at the time, it seems odd that the company would gamble
everything on a vaccine project that was
opposed
by the few investors that were still willing to fund Moderna in
January/February 2020.
Why would they divert their scant resources towards a
project born only out of Barney Graham's "musings" that Moderna could
try to test the speed of its vaccine development capabilities and Bancel's
doomsday view that a "biblical plague" was imminent, especially when
their investors opposed the idea?
Moderna Gets
to Bypass Its Long-Standing Issues With R & D
Moderna produced the first batch of its COVID-19 vaccine
candidate on February 7, one month after Bancel and Graham's initial
conversation. After a sterility test and other mandatory tests, the first batch
of its vaccine candidate, called mRNA-1273, shipped to the NIH
on February 24. For the first time in
a long time, Moderna's stock price surged. NIH researchers administered
the first dose of the candidate into a human volunteer less than a month later,
on March 16.
Controversially, in order to begin its human trial on March
16, regulatory agencies had to allow Moderna to bypass major aspects of
traditional animal trials, which many experts and commentators noted was highly
unusual
but was now deemed necessary due to the urgency of the crisis. Instead of
developing the vaccine in distinct sequential stages, as is the custom, Moderna
"decided to do all of the steps [relating to animal trials] simultaneously."
In other words, confirming that the candidate is working
before manufacturing an animal-grade vaccine, conducting animal trials,
analyzing the animal-trial data, manufacturing a vaccine for use in human
trials, and beginning human trials were all conducted simultaneously by
Moderna. Thus, the design of human trials for the Moderna vaccine candidate was
not informed by animal-trial data.
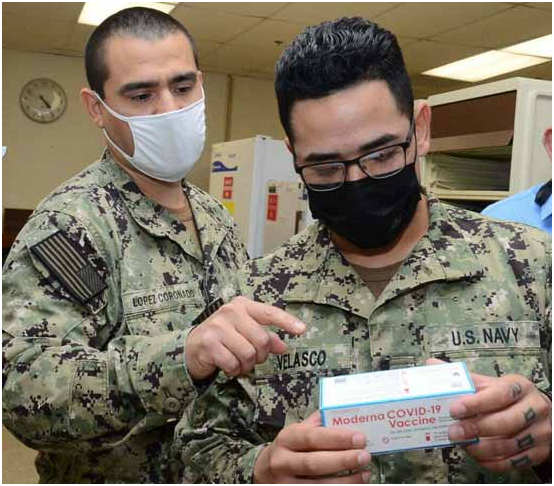
Lt. Javier Lopez Coronado and Hospitalman Francisco Velasco
inspect a box of COVID-19 vaccine vials at the Naval Health Clinic in Corpus
Christi, TX, December 2020; Source: Wikimedia
This should have been a major red flag, given Moderna's
persistent difficulties in getting its products past animal trials. As noted in
Part
I,
up until the COVID-19 crisis, most of Moderna's experiments and products had
only been tested in animals, with only a handful able to make it to human
trials.
In the case of the Crigler-Najjar therapy that it was forced
to indefinitely delay, toxicity concerns related to the mRNA delivery system
being used had emerged in the animal trials, which Moderna was now greenlighted
to largely skip. Given that Moderna had subsequently been forced to abandon all
multidose products because of poor results in animal trials, being allowed to
skip this formerly insurmountable obstacle was likely seen as a boon to some at
the company.
It is also astounding that, given Moderna's history with
problematic animal trials, more scrutiny was not devoted to the regulatory
decision to allow Moderna to essentially skip such trials. Animal studies
conducted on Moderna's COVID-19 vaccine did identify problems that should have
informed human trials, but this did not happen because of the regulatory decision.
For example, animal reproductive toxicity studies on the
Moderna COVID-19 vaccine that are cited by the European Medicines Agency found
that there was reduced fertility in rats that received the vaccine (e. g.,
overall pregnancy index of 84.1% in vaccinated rats versus 93.2% in the
unvaccinated) as well as an increased proportion of aberrant bone development
in their fetuses.
That study has
been criticized for failing to report on the accumulation of vaccine in the
placenta as well as failing to investigate the effect of vaccine doses
administered during key pregnancy milestones, such as embryonic organogenesis.
In addition, the number of animals tested is unstated, making the statistical
power of the study unknown.
At the very least, the 9 percent drop in the fertility index
among vaccinated rats should have prompted expanded animal trials to
investigate concerns of reproductive toxicity before testing in humans.
Yet, Moderna declined to further investigate reproductive
toxicity in animal trials and entirely excluded reproductive toxicity studies
from its simultaneous human trials, as pregnant women were excluded from
participation in the clinical trials of its vaccine. Despite this, pregnant
women were labeled a priority group for receiving the vaccine after Emergency
Use Authorization (EUA) was granted for the Moderna and Pfizer/BioNTech
vaccines.
Per the New
England Journal of Medicine, this meant that "pregnant women and their clinicians
were left to weigh the documented risks of Covid-19 infection against the
unknown safety risks of vaccination in deciding whether to receive the
vaccine."
Moderna only began recruiting for an "observational
pregnancy outcome study" of its COVID-19 vaccine in humans in mid-July
2021, and that study is projected to
conclude
in early 2024. Nevertheless, the Centers for Disease Control recommends the use of
Moderna's COVID-19 vaccine in "people who are pregnant, breastfeeding,
trying to get pregnant now, or might become pregnant in the future."
This recommendation is largely based on the CDC's publication of
preliminary data on mRNA COVID-19 vaccine safety in pregnant women in June
2021, which is based on passive reporting systems in use within the United
States (i. e., VAERS and v-safe).
Even in the limited scope of this study, 115 of the 827
women who had a completed pregnancy during the study lost the baby, 104 of
which were spontaneous abortions before 20 weeks of gestation. Of these 827
pregnant women, only 127 had received a mRNA vaccine before the 3rd trimester.
This appears to suggest an increased risk among those women
who took the vaccine before the 3rd trimester, but the selective nature of the
data makes it difficult to draw any definitive conclusions.
Despite claims from the
New England Journal of Medicine that the study's data was
"reassuring", the study's authors ultimately stated that their study,
which mainly looked at women who began vaccination in the third trimester, was
unable to draw "conclusions about spontaneous abortions, congenital
anomalies, and other potential rare neonatal outcomes."
This is just one example of the problems caused by
"cutting corners" with respect to Moderna's COVID-19 vaccine trials
in humans and animals, including those conducted by the NIH.
Meanwhile, throughout February, March and April, Bancel was
"begging
for money"
as Moderna reportedly lacked "enough money to buy essential ingredients
for the shots" and "needed hundreds of millions of dollars, perhaps
even more than a billion dollars" to manufacture its vaccine, which had
only recently begun trials. Bancel, whose tenure at Moderna had long been
marked by his ability to charm investors, kept coming up empty-handed.
Then, in mid-April 2020, Moderna's long-time cooperation
with the US government again paid off when Health and Human Services Biomedical
Advanced Research and Development Authority (BARDA) awarded the company $483
million
to "accelerate the development of its vaccine candidate for the novel
coronavirus."
A year later, the amount invested in Moderna's COVID-19
vaccine by the US government had grown to about
$6 billion dollars, just $1.5 billion short of the company's entire value at
the time of its pre-COVID IPO.
BARDA, throughout 2020, was directly overseen by the HHS
Office of the Assistant Secretary for Preparedness and Response (ASPR), led by
the extremely
corrupt Robert Kadlec, who had spent roughly the last two decades designing BARDA
and helping shape legislation that concentrated many of the emergency powers of
HHS under the Office of the ASPR.
Conveniently, Kadlec occupied the powerful role of ASPR that
he had spent years sculpting at the exact moment when the pandemic, which he
had simulated the previous year via Crimson Contagion, took place. As mentioned
in Part
I,
he was also a key participant in the June 2001 Dark Winter exercise.
In his capacity as ASPR during 2020, Kadlec oversaw nearly
all major aspects of the HHS COVID-19 response and had a
key role in BARDA's funding decisions during that period, as well as in the
affairs of the NIH and the Food and Drug Administration as they related to
COVID-19 medical countermeasures, including vaccines.
On May 1, 2020, Moderna announced a ten-year manufacturing
agreement with the Lonza Group, a multinational chemical and biotech company
based in Switzerland. Per the agreement, Lonza would build out vaccine
production sites for Moderna's COVID-19 vaccine, first in the US and
Switzerland, before expanding to Lonza's facilities in other countries.
The scale of production discussed in the agreement was to
produce 1 billion doses of Moderna's COVID-19 vaccine annually. It was claimed
that the ten-year agreement would also focus on other products, even though it
was well known at the time that other Moderna products were "nowhere
close to being ready for the market."
Moderna executives would
later state that they were still scrambling for the cash to manufacture
doses at the time the agreement with Lonza was made.
The decision to forge a partnership to produce that quantity
of doses annually suggests marvelous foresight on the part of Moderna and Lonza
that the COVID-19 vaccine would become an annual or semiannual affair, given
that current claims of waning immunity could not have been known back then
because initial trials of the Moderna vaccine had begun less than two months
earlier and there was still no published data on its efficacy or safety.
However, as will be discussed Part III of this series,
Moderna needs to sell "pandemic level" quantities of its COVID-19
vaccine every year in order to avoid a return of the existential crises it
faced before COVID-19 (for more on those crises, see Part
I).
The implications of this, given Moderna's previous inability
to produce a safe product for multidosing and lack of evidence that past issues
were addressed in the development of its COVID-19 vaccine, will also be discussed
in Part III of this series.
It is also noteworthy that, like Moderna, Lonza as a company and its leaders are closely
affiliated with the World Economic Forum. In addition, at the time the
agreement was reached in May 2020, Moncef Slaoui, the former GlaxoSmithKline
executive, served on the boards of both Moderna and Lonza.
Slaoui withdrew from the boards of both companies two weeks
after the agreement was reached to become the head of the US-led
vaccination-development drive Operation Warp Speed. Moderna
praised
Slaoui's appointment to head the vaccination project.
By mid-May, Moderna's stock price — whose steady decline
before COVID-19 was detailed in Part
I
— had tripled since late February 2020, all on high hopes for its COVID-19
vaccine.
Since Moderna's stock had begun to surge in February, media
reports noted that "nearly every progress update — or media
appearance by Moderna CEO Stephane Bancel — has been gobbled up by investors,
who seem to have an insatiable appetite for the stock."
Bancel's tried-and-tested method of keeping Moderna afloat
on pure hype, though it was faltering before COVID-19, was again paying off for
the company thanks to the global crisis and related panic.
Some critics did emerge, however, calling Moderna's now $23
billion valuation "insane,"
especially considering that the company had posted a net loss of $514 million
the previous year and had yet to produce a safe or effective medicine since its
founding a decade earlier.
In January 2020, Moderna had been worth a mere $5 billion,
$2 billion less than its valuation at its December 2018 IPO. If it hadn't been
for the onset of the COVID crisis and a fresh injection of hype, it seems that
Moderna's valuation would have continued to shrink.
Yet, thankfully for Moderna, investors were valuing
Moderna's COVID-19 vaccine even before the release of any clinical data. Market
analysts at the time were
forecasting Moderna's 2022 revenue at about $1 billion, a figure based
almost entirely on coronavirus vaccine sales, since all other Moderna products
were years away from a market debut.
Yet, even with this forecasted revenue, Moderna's stock
value in mid-May 2020 was trading
at twenty-three times its projected sales, a phenomenon unique to Moderna among
biotech stocks at the time. For comparison, the other
highest multiples in biotech at the time were Vertex Pharmaceutical and
Seattle Genetics, which were then trading at nine and twelve times their
projected revenue, respectively.
Now, with the implementation of booster shot policies around
the world, revenue forecasts for Moderna now predict the company will make a
staggering $35
billion
in COVID-19 vaccine sales through next year.
Moderna's surging stock price went into overdrive when, on
May 18, 2020, the company published "positive" interim data for a
phase 1 trial of its COVID-19 vaccine. The results generated great press,
public enthusiasm, and a 20 percent boost in Moderna's stock price.
Just hours
after the press release, Moderna announced a new
effort to raise $1.3 billion by selling more stock. It has since been revealed
that that Moderna had hired Morgan Stanley to manage that stock sale on
May 15.
However, left largely unmentioned by the press or Moderna
itself was that the ostensibly "scientific study" only provided data
from 8 of the 45 volunteers — 4 volunteers each from the 15- and 100-microgram
dose cohorts — regarding the development of neutralizing antibodies.
The age of these mysteriously selected 8 volunteers was also
not published, and other key data was missing, making
it
"impossible to know whether mRNA-1273 [Moderna's COVID-19 vaccine] was
ineffective [in the remaining 37 volunteers whose antibody data was not
disclosed], or whether the results were not available at this point."
Meanwhile, in the highest-dose cohort, in which volunteers
received 250 micrograms, 21 percent of volunteers experienced a grade 3 adverse
event, which is defined by the FDA as "preventing daily activity and
requiring medical intervention."
STAT published
a report
the next day that was skeptical of Moderna's press release and seemed to imply
the data release was aimed at boosting the company's stock valuation, which hit
$29 billion after the news. STAT reporter Helen Branswell called this jump in
valuation "an astonishing feat for a company that currently sells zero
products."
Branswell's report noted several things, including that
several vaccine experts had noted that "based on the information made
available [by Moderna], there's really no way to know how impressive — or not —
the vaccine may be."
Moderna later
defended
its withholding of key data in the press release, claiming that it was done to
respect "federal securities laws and the rules of scientific
journals" and to prevent a potential leak of the data from insiders at the
NIH.
Moderna executives have
more recently claimed that the "timely" release of these selective data
had been linked to their "desperate" fundraising efforts at the time
and ultimately prevented them from "losing" the COVID-19 vaccine
race.
The STAT report also noted that the National Institute of
Allergy and Infectious Diseases (NIAID), which was running the trial referenced
by Moderna in the press release, was completely silent on the matter, declining
to put out a press release that day and declining to comment on Moderna's
announcement.
This was described as uncharacteristic for NIAID, especially
considering they were the part of the NIH co-developing the vaccine with
Moderna and running the trial. STAT noted that, normally, "NIAID doesn't
hide its light under a bushel. The institute generally trumpets its
findings." In this case, however, they declined to do so.
It emerged in early June 2020 that Dr. Anthony Fauci, who
leads NIAID, had been displeased with Moderna's decision to publish incomplete
data on the trial, telling
STAT
that he would have preferred "to wait until we had the data from the
entire Phase 1 ... and publish it in a reputable journal and show all the
data."

Tal Zaks, Chief Scientific Officer at Moderna; Source: The
Forward
It subsequently emerged that Moderna's top executives,
including chief financial officer Lorence Kim and chief scientific officer Tal
Zaks, had
used their insider knowledge of the coming press release to
trade company stock that netted them several million each following the jump in
Moderna's stock that resulted from the press release's positive buzz.
A little over a week after the press release had been published,
STAT
reported
that the top five Moderna executives had cashed out $89 million in shares since
the company's stock price had begun to soar earlier in the year.
Per that report, the amount of trades by these five
executives alone between January and May 2020 was "nearly three times as
many stock transactions than in all of 2019." By September 2020, the
amount of stock shed by Moderna executives amounted to $236
million.
Less criticized or even mentioned by the press was Moderna's move, less than a
month later, to create
a tax haven in Europe for its European COVID-19 vaccine sales.
Though the trades were deemed slimy but legal, mainstream
media reports essentially
confirmed
that the early release of the interim data was planned to "raise the share
price of Moderna's stock so that executives could cash in during the period of
euphoria" that followed. Some
watchdog groups called on the SEC to investigate Moderna executives for
manipulating the stock market.
The critical reporting on executive stock trades and
Moderna's release of incomplete data led the company's stock to temporarily trend
downward
throughout the rest of May. As previously mentioned, Moderna has repeatedly
attempted to explain away the timing of this particular press release, offering
new explanations as recently as this
week.
Moderna's
Shocking Claim About Its Vaccine Candidate
In mid-June 2020, researchers at the NIH and Moderna published
a manuscript preprint of preclinical data for Moderna's COVID-19 vaccine. This
preprint described the vaccine as employing a delivery system covered in a
patent owned by the company Arbutus Biopharma and described the results of that
vaccine in tests on mice.
As discussed in Part
I,
Moderna has long been locked in a bitter legal dispute with Arbutus, which has
threatened Moderna's ability to ever turn a profit on any product that relies
on Arbutus-patented technology regarding lipid nanoparticle (LNP) delivery
systems for its mRNA products. Moderna has claimed for years it was no longer
using the Arbutus-derived system on which it once entirely relied, with Bancel
even going so far as to publicly call it "not very good."
However, Moderna has provided no real evidence that it no
longer relies on the technology covered in the Arbutus patents. The June 2020
manuscript preprint from the NIH and Moderna provided evidence indicating that
the same Arbutus-derived technology that had caused major toxicity issues in
multidose products Moderna had previously attempted to develop was also being
used in Moderna's COVID-19 vaccine candidate.
Yet, when Moderna's chief corporate affairs officer, Ray
Jordan, was challenged on this point by
Forbes,
Jordan asserted that the preprint's data had been generated using a formulation
of a COVID-19 vaccine that is not the same as the vaccine itself, stating,
"while the authors of the preprint used the term 'mRNA-1273' for
convenience of the reader, the preprint does not describe the cGMP process by
which we make our messenger RNA and LNP or the final drug product composition
in our commercial candidate (mRNA-1273)."
When Forbes asked Jordan if he could provide any specifics,
including the LNP molar ratio of the new LNP technology to prove that the LNPs
in use in the COVID-19 vaccine were in fact different from those covered by the
Arbutus patent, Jordan flat out refused.

Arbutus Biopharma's office in Warminster, Pennsylvania;
Source: Philadelphia
Business Journal
Despite Jordan's claims, a Moderna preclinical study
regarding its COVID-19 vaccine was published a month
later,
and that July study noted that the Moderna vaccine used LNPs as described in a
2019 paper, which in turn reveals that the LNPs in question were the same as
those used in the June study. This paper included the results from the study
originally promoted by Moderna in May that led to a jump
in Moderna's stock price.
Now published in full, the study generated lots of positive
press, including a statement from the
NIAID's Fauci that "no matter how you slice this, this is good news."
A jump in US government funding of Moderna's COVID-19 vaccine also
shortly followed the study's publication.
At the time, CBS
News remarked that Moderna's stock price, which had been sliding since
its late 2018 IPO, had been essentially rescued by the COVID-19 crisis, as
"shares of Moderna — which has never brought a product to market over its
ten-year existence — have soared as much as 380 percent since the start of the
year as news emerged [in January] of its promising potential for producing a
vaccine.
[Moderna's] stock price was less than $20 in early January
and around $95 on Friday [July 17, 2020]." Today, by comparison, Moderna
has consistently been trading above $300 a share.
Yet, if we take Ray Jordan at his word with respect to the
preprint published in June, Moderna appears to have been engaged in rather
slimy behavior. If Jordan was telling the truth, it appears that this July
study, which appears to use the vaccine candidate containing the same LNPs as
those described in the June 2020 preprint, also used a formulation not
consistent with the company's commercial vaccine candidate.
If so, given that the July study was the same study referenced
by Moderna's controversial May press release tied to insider stock trades,
Moderna appears to have used "positive" data generated by a vaccine
candidate other than its commercial vaccine candidate to boost stock prices and
ameliorate the company's financial situation while also generating millions for
executives.
This, of course, says nothing about the separate but
critically important issue that the vaccine candidate used in these studies,
including the NIH study, is
not necessarily the same as the commercial candidate used in clinical trials.
It seems that the only reason that Moderna would make such
an outrageous claim to Forbes would be to distance its COVID-19 vaccine from
its past controversies that largely have their root in Moderna's LNP-related
problems, which it had claimed to have already resolved. It is not clear if the
motive behind such a gambit is principally related to the legal dispute with
Arbutus or the past safety issues Moderna encountered with multidose therapies.
Adding to the confusion about the LNPs in use in Moderna's
products is that, a few days earlier in July, Moderna had published
results
on a separate vaccine candidate, this one for HIV, that appeared to use the
exact same LNP technology that is covered by the Arbutus patent. The LNPs
described in that study included the same components as those described in the
Arbutus patent and the same molar ratio.
Moderna appeared
to be referencing this issue in their August 6, 2020, SEC filing, which
states: "There are many issued and pending third-party patents that claim
aspects of oligonucleotide delivery technologies that we may need for our mRNA
therapeutic and vaccine candidates or marketed products, including mRNA-1273,
if approved."
By the end of 2020, Moderna claimed in a
December filing with the SEC that, while it had "initially
used LNP formulations that were based on known lipid systems," that is,
the Arbutus LNPs, it had "invested heavily in delivery science and ha[s]
developed LNP technologies, as well as alternative nanoparticle
approaches."
Despite the claims it made in this filing, however, it
remained unclear as to whether the company's COVID-19 vaccine was using Arbutus
technology or the technology it purported to have developed on its own without
infringing on Arbutus's intellectual property.
Moderna's claims that it now uses a different LNP system
than the one that caused such major issues is based on the company's
development and implementation of a lipid structure now known as SM-102. This
lipid structure was first revealed by Moderna in a 2019
publication under the name Lipid H, and, in that paper and since,
Moderna has claimed that its LNP system is now superior to that which it
previously used because it is using SM-102 instead of the original Arbutus
lipids.
However, it is critical to note that Moderna's use of SM-102
does not necessarily mean the company is not violating the Arbutus patents,
which cover the use of LNPs that combine cationic and PEGylated lipids in
specific proportions.
Despite claims from Moderna that SM-102 resolved both the
company's patent-related and toxicity issues with its LNP system (as discussed
in Part
I),
Moderna has declined
to disclose SM-102's exact structure or whether it carries a net
positive charge at physiological pH, the latter of which could lead to proof of
continued infringement on the Arbutus patent.
In addition, there are no studies on the distribution,
degradation, and/or elimination of SM-102 from the body, meaning that the
accumulation of the lipids or their capacity to damage organs is not
documented.
The obvious lack of study of SM-102's properties and effects
on the human body was largely circumvented by public health authorities during
the emergency approval process by using the same criteria for the Moderna
vaccine candidate that is used for traditional vaccines that do not utilize the
novel mRNA approach. These "traditional" criteria therefore do not
include any requirements for data on LNP safety.
Overall, the evidence seems to point toward Moderna's claims
that its COVID-19 vaccine doesn't use Arbutus-derived LNPs as being false. The
other possibility is that Moderna attempted to modify the LNP system but only
slightly so that potential identifiers, such as the molar ratio, remained the
same.
In this case, Arbutus could still claim that the LNPs currently
in use by Moderna and in its COVID-19 vaccine infringe on their patent. It is
also thus likely that the safety issues Moderna had acknowledged with this LNP
system were largely unaffected if the potential modifications were indeed
minor.
Yet, if either of these scenarios is correct, the question
becomes – Why wouldn't Arbutus challenge Moderna once again to obtain royalty
payments stemming from its COVID-19 vaccine?
The answer seems to lie mostly in optics and public
relations. As STAT
wrote
last July, were Arbutus to sue Moderna over patent infringement in the midst of
the COVID-19 crisis, "that would mean taking the substantial risk that it
would be perceived as a company holding up a desperately needed medicine out of
concern for its bottom line."
This also seemed to be part of the motive behind Moderna's altruistically
framed promise not to enforce its own COVID-19–related patents until the
pandemic is declared over.
Observers have noted that this move by Moderna was not only
a public relations boon for the company but also "set a disarming tone in
the space that may serve to deter others in the space [e.g., Arbutus] from
acting too defensively or aggressively," largely due to "fear of the
potential public relations backlash."
While July 2020 brought a surge in valuation and positive
press for Moderna and its COVID-19 vaccine candidate, it also brought an
unfavorable ruling for Moderna in its long-running dispute with Arbutus, one
that opened the door for Arbutus to file an injunction against Moderna's
COVID-19 vaccine, if they chose, to force the negotiation of a license with
Moderna.
The news led to Moderna's stock price falling by 10 percent,
wiping out $3 billion in value. However, most likely for the reasons outlined
above, Arbutus ultimately declined to jump on the decision to block Moderna's
COVID-19 vaccine from advancing in the hopes of securing royalties. Yet, they
reserve the ability to do so, if and when the perceived urgency of the COVID-19
crisis fades.

Ray Jordan, Chief Corporate Affairs Officer at Moderna;
Source: PRSA
Moderna has asserted that the decision would not affect its
COVID-19 vaccine as the company was "not aware of any significant
intellectual property impediments for any products we intend to
commercialize."
Thus, Ray Jordan's assertions and the lack of "clear
and convincing" evidence that Moderna's COVID-19 vaccine relies on
Arbutus-patented technology appears to have been sufficient for Moderna to make
this claim.
This seems to be due to a lack of interest by the mainstream
media or federal agencies/regulators in demanding concrete evidence that
Moderna's LNP system used in its COVID-19 vaccine does not rely on
Arbutus-patented technology.
Despite the issues raised above in relation to the vaccine
study data published in June and July, the positive press attention —
particularly after the July publication — translated just a month later into
the US government entering
into a significant supply agreement with Moderna on August 11, 2020.
Per that agreement, the government would pay $1.525 billion
for 100 million doses with the option to purchase an additional 400 million
doses in the future, all of which it has since
purchased.
Per Moderna's press release, the agreement meant that the US government had, by
that point, paid $2.48 billion for "early access" to Moderna's
COVID-19 vaccine.
Roughly a month later, it was revealed that the US
government had been paying for much more. On September 10, 2020, BARDA
joined
long-time Moderna funder and "strategic ally" DARPA in scrutinizing
contracts that had been awarded to the company due to Moderna's failure to
disclose the role government support had played in its numerous patent
applications.
The announcement came after Knowledge Ecology International
(KEI), which advocates for protecting taxpayer investments in patents, found
that none
of the patents or applications assigned to Moderna in the
company's entire history had disclosed the considerable US government funding
it had received at the time those patents were filed, which is required by the
1980 Bayh-Doyle Act and by the regulations of the Patent and Trademark Office.
Per KEI, this translates into the US government owning
certain rights over the patents, and thus US taxpayers may have an ownership
stake in vaccines made and sold by Moderna.
Despite the clear evidence that Moderna failed to disclose
the considerable amount of US government funding prior to and during the COVID
crisis in its patent applications, Moderna responded to KEI and the BARDA/DARPA
"scrutiny" by
stating
that it was "aware of and consults with our agency collaborators regarding
our contractual obligations under each of these agreements, including those
with respect to IP [intellectual property], and believe we comply with those
obligations."
As of the writing of this article, BARDA and DARPA have
taken no action against Moderna for their illegal omission about having
received substantial government funding in their patent applications and
filings.
Instead, a month after DARPA claimed to be
"scrutinizing" Moderna's patent applications, it
awarded
the company up to $56 million to develop small-scale mobile means of
manufacturing its products — namely, its COVID-19 vaccine and its personalized
cancer vaccine.
Moderna:
"Just Trust Us"
What quickly stands out about Moderna's COVID-19 vaccine
candidate over the course of its rapid development in 2020 was the willingness
of federal agencies like NIH, BARDA, and others, as well as the mainstream
press, to take Moderna at its word concerning critical aspects of its vaccine
and its development, even when the evidence appeared to contradict its claims.
This is particularly evident in Moderna claiming that it
resolved its
LNP issues, both in terms of toxicity and patent infringement, and
those claims — despite the company's refusal to release clear supporting
evidence — being taken at face value.
This is even more striking when one considers the multiple
factors that Moderna was facing before
COVID-19
and how the company faced
collapse
without the success of its COVID-19 vaccine, as this means Moderna was under
considerable pressure to have its vaccine succeed.
While the controversial simultaneous conducting of animal
and human trials was publicly justified in the name of the urgency of the
COVID-19 crisis, can the other examples explored in this article be similarly
justified in the name of urgency? Instead, several issues explored above appear
to have been driven by conflicts of interest and corruption.
Adding to the ridiculousness is that Moderna got away with
claiming that the NIH was conducting safety tests on a COVID-19 vaccine product
different from their commercial candidate, without causing a major backlash in
either the mainstream media or from the NIH itself.
This is particularly telling as the May 2020 press release
and suspiciously timed stock trading by Moderna executives and insiders did
garner negative press attention.
However, the subsequent revelation, per Moderna, that its
press release was based on the study of a vaccine candidate that was not
"necessarily the same" as their commercial COVID-19 vaccine candidate
received essentially no coverage, despite raising the unsettling possibility
that Moderna could have used another product to essentially rig preliminary
data to be positive in order to advance their product to market and make
millions through insider stock sales.
How can the claims made by such a company be trusted at face
value without independent verification? Furthermore, how can NIH studies of
Moderna be trusted when Moderna has claimed that some of the studies that were
ultimately factors in the vaccine's emergency use authorization approval by the
FDA utilized a different product than that which Moderna later successfully
commercialized?
Moderna and the NIH were,
nevertheless, taken at their word in November 2020 when they said
that their COVID-19 vaccine candidate was 94.5 percent effective. At the time,
the main
promoters
of this claim were Moderna's Bancel and NIAID's Fauci.
The claim came shortly after Pfizer's press release claiming
its COVID-19 vaccine candidate was
90 percent effective. Not to be outdone by Moderna, Pfizer revised the
reported efficacy of its vaccine just two days after Moderna's November press
release, stating that their vaccine was actually 95% effective to Moderna's
94.5%.
In the case of these claims, it was indicative of the
now-established yet troubling practice of "science by press release"
when it comes to touting the benefit of certain COVID-19 vaccines currently on
the market. Since then, real-world data has
shattered
the efficacy claims that were used to secure emergency use authorization, for
which Moderna applied at the end of November 2020 and received only a few weeks
later in mid-December of that year.
As Part III of this series will explore, the EUA for the
Moderna vaccine got around the issues raised in this article by treating the
entire Moderna formulation as a traditional vaccine, which it is not, as
traditional vaccines do not utilize mRNA for inducing immunity, and their
safety and efficacy depend on several criteria that are entirely different from
those of the more novel mRNA.
Thus, the LNP issue, a perpetually sticky one for Moderna
that it struggled to circumvent before the onset of the COVID-19 crisis, was
largely evaded when it came down to, not just research and development, but
receiving EUA.
It appears that this sleight-of-hand by federal regulators
was necessary for Moderna, after ten years, to finally get its first product on
the market. As noted in Part
I,
were it not for the COVID-19 crisis and its fortuitous timing, Moderna might
not have survived the severe challenges that threatened its entire existence as
a company.
Part III will also examine how Moderna's "Hail
Mary" moment in the COVID-19 crisis was only the beginning of its
miraculous rescue from a Theranos-like fate, as the company has not only
expanded its partnership with the government but now with a CIA-linked firm.
This shows that Moderna and key power players in Big Pharma
and the US national-security state envision Moderna's COVID-19 vaccine being
sold in massive quantities for several years to come. As previously noted,
without annual or semiannual sales of booster doses, Moderna's pre-COVID crisis
will inevitably return.
The push for Moderna booster-dose approval has advanced
despite real-world data not supporting Moderna's past claims of safety and
efficacy for its COVID-19 vaccine, the recent decision of several European
governments to halt the vaccine's use, and the FDA's own infighting and recent
admissions that the Moderna COVID-19 vaccine is one
of the more dangerous currently in use, particularly in terms of adverse effects
on the cardiovascular system.
The obvious question here then becomes – How costly will
Moderna's "Hail Mary" save ultimately be, not just in terms of the $6
billion US taxpayer money already spent on it, but also in terms of public
health?
+
Will the Military Industrial Complex Permit Good Relations
Between the U.S. and China?
http://www.informationclearinghouse.info/56865.htm
by Brian
Cloughley
===========
e.
CREEPY PFIZER AD TO ENCOURAGE CHILDREN
TO TAKE THE COVID-19 VACCINE
https://odysee.com/@RealNewsforever:a/Pfizer-Vaccine-Ad-Targets-Children:5
by Real
Newsforever
(1:28)
This ad was produced by Pfizer.
The FDA vaccine advisory panel voted almost unanimously
on Tuesday, November 2 recommending the vaccination of young children with the
Covid-19 vaccines.
The FDA accepted that recommendation and approved the Covid-19 vaccinations for
children 5-11. This is in spite of the fact that the CDC reports 474 deaths for
the age group 5 to 18 from Covid-19 from 1-4-2020 to 10-30-2021.
https://data.cdc.gov/NCHS/Provisional-COVID-19-Deaths-Focus-on-Ages-0-18-Yea/nr4s-juj3
The approval of the Covid-19 vaccine for children as
young as 5 is insane, unnecessary and proves that Big Pharma, the FDA, the CDC
and the Public Health special interest have too much power
Many children die from accidents each year than have died
of Covid-19.
+
#Heineken #SocialiseResponsibly
Heineken
| The Night is Young
https://www.youtube.com/watch?v=akxfPV-A_C0
(1:03)
578K subscribers
These recent months we’ve had to give up the simple
moments we used to take for granted, like enjoying a beer with friends. We want
to celebrate people's resilience and inventiveness to keep going and say...
keep it up!
“We will meet each other again.”
These recent months we’ve had to give up the simple moments
we used to take for granted, like enjoying a beer with friends. We want to
celebrate people's resilience and inventiveness to keep going and say... keep
it up!
Click here for more: https://www.youtube.com/user/heineken Follow Heineken on Instagram: https://www.instagram.com/heineken/ Follow
Heineken on Twitter: https://twitter.com/heineken
+
Britons
Sing About Where To Stick Their Poison Vaccines
https://www.bitchute.com/video/NvI4Er74uIqq/
(00:59)
===========
f.
The Great Heart Disease Cover-up, Long-Haul Illusion Exposed
&
Your Endless Booster Future Admitted
with Ryan
Cristián
(3:19:06)
+
Steve
Kirsch presents to FDA:
Age
5-11 Review Board on EUA Pfizer Vaccines
https://odysee.com/@VSRF:d/Steve-Kirsch-clip-FDA-presentation:1
(3:26)
Steve Kirsch, Speaks to FDA Vaccine Committee regarding
the EUA Review for Ages 5-11-year-olds. Serious data signals concerning
children exist. Why are children dropping like flies after the vaccine? How can
a healthy 16-year-old drop dead during a Math Zoom class? Why did a 15-year-old
die in his sleep? How were all these safety signals missed including Pulmonary
Embolism, Thrombosis, Myocarditis, Ischaemic stroke, DVT? Questions you need to
ask before approving this EUA.
See Full FDA VRBPAC Panel Discussion: Vaccines and
Related Biological Products Advisory Committee 10/26/21 here: https://youtu.be/laaL0_xKmmA
See Slides for FDA VRBPAC Committee presentation: https://www.skirsch.com/covid/VRBPAC-10-26-21.pdfSee Steve Kirsch Presentation: False Narrative Takedown
Series, Covid Vaccines have killed over 200,000 Americans https://rumble.com/vm8ayu-tfnt-1-covid-vaccines-have-killed-over-200000-americans.html
Who is Steve Kirsch?
Steve Kirsch is Executive Director of the Covid-19 Early Treatment Fund and is
the CEO of the M10 Networks, which develops digital money technology for banks
and central banks. He is the inventor of the optical mouse and one of the first
Internet search engines, Infoseek. As the founder of 7 high tech companies, two
with billion-dollar market caps, Steve is focused on modernizing payment
infrastructure. He has a BS/MS in Electrical Engineering and Computer Science
from MIT.
#covid19earlytreatmentfund #kirsch #fda #fdapanel
#heartattacks #vaccines #vaccinereactions #pfizer #news #covid19 #today
#fdavrbpac #maddiedegaray #teenvaccines #covidvaccines ##myocarditis
#pericarditis #myocarditisvaccines #vsrf #myocarditisvaccine #vrbpac
+
Top 1% Gains More Wealth Than GDPs Of Japan, Germany, UK, France,
India, & Italy Combined;
Bottom 50% - You Get Nothing
by Charles Hugh Smith via OfTwoMinds blog
+
Food
as a Weapon: Starving Us into Submission
https://www.globalresearch.ca/food-weapon-starving-us-submission/5761613
by S. M. Smyth
===========
g.
Applying brakes on 'Warp Speed'
COVID-19 vaccinations for children
https://m.washingtontimes.com/news/2021/oct/28/applying-brakes-on-warp-speed-covid-19-vaccination/
by Dr.
Larry Kwak, Dr. Steven T. Rosen and Dr. Idit Shachar
October 28,
2021
+
Vaccine Development and Social Control: A Psychopathology of Impaired
Reasoning in the
Global Push for Mass Compliance
https://ijvtpr.com/index.php/IJVTPR/article/view/29/55
by Daniel Broudy
+
OSHA Suspends Biden’s Employer Vaccine Mandates Following
Court Order
===========
h.
From: Children's Health Defense
[mailto:team@childrenshealthdefense.org]
Sent: Saturday, November 13, 2021 2:33 AM
To: Francis Feeley
Subject: 112 Kids Get Wrong COVID Vaccine + 21 Studies Proving Vaccine
Mandates Not Science-Based + More
|














===========
i.
From: The Grayzone
[mailto:grayzoneproject@gmail.com]
Sent: Sunday, November 14, 2021 5:24 PM
To: francis.feeley@wanadoo.fr
Subject: From Nicaraguan revolutionaries to US embassy informants: How
Washington recruited ex-Sandinistas like Dora María Téllez and her MRS party
|




+
Antiwar.com
+
Selected
Articles at Global Research
November 18,
2021
===========
j.
Treating
Long-Haul Syndrome
https://www.vax.guide/2021/11/20/treating-long-haul-syndrome/
with Dr. Al
Johnson and Dr. Peter McCullough
(41:29)
Story
at-a-glance
- Long-haul
syndrome refers to symptoms that persist for four or more weeks after an
initial COVID-19 infection
- Board-certified
internist and cardiologist and editor of two medical journals Dr. Peter
McCullough discusses potential treatments for long-haul syndrome
- McCullough
uses full-dose aspirin — 325 milligrams a day — in almost everyone with
long COVID syndrome who doesn’t have a major blood clot, in addition to
other medications
- A
better alternative to aspirin is digestive fibrinolytic enzymes like
lumbrokinase and serrapeptase; anyone who had COVID-19, especially with
significant symptoms, should consider taking digestive fibrinolytic
enzymes to be sure you don’t have any clotting
- An
alternative to determine if clotting is occurring is a test called
D-dimer, although it can be pricey
- FLCCC’s
I-RECOVER protocol can be downloaded in full, giving you step-by-step
instructions on how to treat long-haul COVID syndrome and/or reactions
from COVID-19 injections
Long COVID,
also known as long-haul COVID, chronic COVID or long-haul syndrome, refers to
symptoms that persist for four or more weeks after an initial COVID-19
infection.1 Board-certified internist and
cardiologist Dr. Peter McCullough discusses potential treatments for long-haul
COVID in the video above,2 including
which tests may be necessary and when to seek emergency medical care.
Many of the
symptoms can also mirror those caused by COVID-19 shots, and McCullough details
the four categories of COVID-19 shot-injury syndromes that he’s seen in his
practice. While anyone can experience long COVID, those who are sick enough to
be hospitalized in the ICU are most often affected.
According to
McCullough, 50% of this group will have manifestations of long COVID syndrome.
“So the sicker someone is, and the longer the duration of COVID, the more
likely they are to have long COVID syndrome. That’s the reason why we like
early treatment. We shorten the duration of symptoms and there’s less of a
chance for long COVID syndrome.”3
Common
Symptoms of Long COVID
Signs and
symptoms of long COVID, which persist for four weeks or more after you’ve been
diagnosed with COVID-19, include:4
|
Fatigue |
Shortness
of breath or difficulty breathing |
|
Cough |
Joint pain |
|
Chest pain |
Memory,
concentration or sleep problems |
|
Muscle
pain or headache |
Fast or
pounding heartbeat |
|
Loss of
smell or taste |
Depression
or anxiety |
|
Fever |
Dizziness
when you stand |
|
Worsened
symptoms after physical or mental activities |
These
symptoms are a result of damage to the following body systems:5
- Pulmonary/lungs
- Immune/allergy
- Mitochondria/energy
system
- Heart
- Central/Peripheral
nervous system
According to McCullough, a paper presented by Dr. Bruce
Patterson at the International COVID Summit in Rome, September 12 to 14, 2021,
showed that in “individuals who’ve had significant COVID illness, 15 months
later the s1 segment of the spike protein is recoverable from human monocytes.”
He added:6
“That means the body literally has been sprayed with the
virus and it spends 15 months, in a sense, trying to clean out the spike
protein from our tissues. No wonder people have long COVID syndrome.”
Be on the
Lookout for Blood Clots for 90 Days
If you’ve had COVID-19, especially if it was a severe case,
be aware that blood clots and heart problems, including heart attack, can occur
for 90 days or more. It’s believed that remnants of the virus remain in the
nervous system, the lungs, the heart and other organs.
If the symptoms include major shortness of breath, cough
with blood in it or pain on one side when you take a deep breath, it could be
due to a late pulmonary embolism or a blood clot going to the lungs. “We’ve
seen this on more than one occasion,” McCullough said.7
In this case, McCullough recommends a chest CT with contrast
and, if a blood clot is found, oral blood thinners for three to six months.
McCullough also uses full-dose aspirin — 325 milligrams a day — in almost
everyone with long COVID syndrome who doesn’t have a major blood clot, in
addition to other medications.
However, a safer and likely equally effective alternative to
aspirin is digestive fibrinolytic enzymes like lumbrokinase and serrapeptase.
You can alternate between the two enzymes — one day take lumbrokinase and the
next take serrapeptase — because you’ll need to be on it for about three months
and you can develop a sensitivity to them over time.
Anyone who had COVID-19, especially with significant
symptoms, should consider taking digestive fibrinolytic enzymes to be sure you
don’t have any clotting. An alternative to determine if clotting is occurring
is a test called D-dimer, although it can be pricey. D-dimer is a protein
fragment produced by the body when a blood clot dissolves.
It’s typically undetectable or present only at very low
levels, buts its level may significantly rise when the body is forming and
breaking down blood clots.8 If your d-dimer test is low, then you don’t need to take
the enzymes. Likewise, if you had a very mild, cold-like case, of COVID-19, you
probably don’t need them.
Aside from a CT scan to rule out pulmonary embolism if
you’re having symptoms and possibly a D-dimer test, McCullough suggests a
high-sensitivity C-reactive protein (CRP) test, which provides a general index
of inflammation. Keep in mind, though, as McCullough said:
“This pursuit of a blood clot is very important. I’ve seen
multiple cases now where blood clots have been missed … this is now almost a
daily occurrence, particularly within the first 90 days after COVID-19. I think
after that period of time it becomes progressively less likely.”
Heart
Problems and Neurological Issues Are Common
Inflammation around the lining of the heart — pericarditis —
and the lining of the lungs — pleuritis — may also occur in long COVID. “The
virus can set up inflammation and the spike protein is in the body, it’s
triggered inflammation and, importantly, that’s really a clinical diagnosis,”
McCullough said.9 He prescribes steroids and colchicine, an anti-inflammatory
drug commonly used for gout to reduce high uric acid, in such cases.
There’s a real risk for heart attack or stroke to occur
without warning in long COVID, so McCullough warns those recovering to “be on
your guard,” especially if you have a heart stent or carotid stenosis.
Neurologic syndromes in long COVID also occur, although they
aren’t well described. Symptoms include joint and muscle pain, headaches, brain
fog and tinnitus (ringing in the ears). Some people also have changes in the
autonomic nervous system, such as elevated heart rate, and sensory
neuropathies, including numbness and weakness in the legs.
McCullough’s host in the video, Dr. Al Johnson, recommends
using a foam roller on your back, three to five times a day, to relax your
nervous system, as well as to relieve rib pain from all the coughing.
McCullough has had some success treating neurologic symptoms with an older SSRI
called fluvoxamine.
Supplements
That Play a Role in Long COVID Syndrome
Dr. Johnson recommends several supplements to support
healing from long COVID. Among them:
- Vitamin
C, because it helps calm down inflammation
- Vitamin
D, for both prevention and long haulers
- Glutathione,
because it helps calm down inflammatory processes
- N-acetylcysteine
(NAC), a precursor to glutathione
McCullough, an enlightened allopathic physician, recognizes
the role that dietary and integrative therapies play in helping people recover
from long COVID:10
“As an allopathic doctor, I’m not skilled in understanding
how to use vitamins and supplements like our integrative, holistic and
naturopathic colleagues, but they’ve played a big role in COVID-19. I’ll just
make the observation that COVID-19 is an enormous catabolic strain … the weight
loss is tremendous.
It is such a strain on the body … we want to avoid sugary
foods. When someone has acute COVID-19 and moves into the long COVID,
post-COVID syndrome, we want to stay away from sugary foods … the sugar seems
to feed the virus. It seems to feed inflammatory processes.”
McCullough has also referred some patients to chiropractors
in his area, noting that “long COVID syndrome, out of all the illnesses we
face, is one for collaborative care, for integrative care. There’s a lot of
elements to it.”11 Likewise, Johnson suggests a combination of physical
therapy and exercise — but not overexercising — to get back normal function of
your musculoskeletal system.
Support a
Healthy Microbiome
Research by Dr. Sabine Hazan has shown that your microbiome
plays an incredible role in COVID-19.12 According
to McCullough, she’s figured out that one reason why certain people within the
same household don’t develop COVID-19 while others do comes down to the gut. A
healthy microbiome score is protective against developing COVID-19.
Bifidobacterium, McCullough notes, is among the leading bacteria that appear to
fight off COVID-19.13
“COVID-19 is clearly a GI syndrome,” he said. SARS-CoV-2
collects in your nose and mouth, and as you swallow it’s introduced to your GI
tract. According to Forbes, Li Tongzeng, deputy director of the respiratory and
infectious diseases department at Beijing You An Hospital, cited research that
SARS-CoV-2 survives longer in the anus and feces than in the respiratory tract.
Due to this, an anal swab may be able to more accurately
detect mild or asymptomatic cases than a nose or throat test.14
Staying away from irritants to the GI tract is important,
and Johnson recommends eating a clean diet with organic food and glass-bottled
spring water, if possible. Eating fermented foods, or taking a high-quality
probiotic, is also essential for gut health, as is avoiding unnecessary
antibiotics usage and processed foods.
Chronic
Fatigue and Sleep Disturbances
Chronic fatigue is a major problem for many with long-haul
COVID, and for this Johnson recommends hyperbaric oxygen therapy (HBOT). One of
the reasons I'm fascinated by HBOT, in particular, is because of its ability to
improve mitochondrial function.15 As Johnson
explained, “Toxins affect the mitochondria … the little engines in our body
that create ATP, which is our energy system.”16
HBOT protects against mitochondrial dysfunction,17 speeding up
the mitochondria and ATP production, which helps increase energy while
decreasing brain fog and fatigue. Further, Johnson added, it helps heal body
tissues like your lungs, heart and muscles while decreasing inflammation and
lessening symptoms.
If sleep disturbances are an issue — and they often are for
long haulers — McCullough recommends avoiding alcohol for at least a month, as
“just one drink in 28 days will destroy sleep architecture.” The Front Line
COVID-19 Critical Care Working Group (FLCCC) has a management protocol —
I-RECOVER18 — for long
haul COVID-19 syndrome that includes melatonin, which can also help with sleep
disturbances.
Shot-Induced
Myocarditis Is Worse Than COVID’s
McCullough detailed the non-fatal syndromes that are
occurring after COVID-19 shots, which cause symptoms similar to that of long
COVID in many cases. The shot-induced syndromes fall into four areas, the first
being cardiac.
Myocarditis is a recognized effect of both COVID-19 and
COVID-19 shots, but they’re completely different, McCullough said. “A child is
more likely to be hospitalized with myocarditis after a Pfizer or Moderna
[shot] than actually being hospitalized with COVID-19,” he said. Further:19
“The myocarditis in COVID-19 is mild. It’s inconsequential.
I don’t want anyone to think that the myocarditis we’re seeing with the natural
infection is anything like what we’re seeing with the [shots] … there are
studies suggesting the lipid nanoparticles actually go right into the heart,
the heart expresses the spike protein, the body attacks the heart.
There are dramatic EKG changes. The troponin, the blood test
for heart injury with the vaccine myocarditis, is 10 to 100 volts higher than
the troponin we see with the natural infection. It’s a totally different
syndrome. When the kids get myocarditis after the vaccine, 90% have to be
hospitalized … so vaccine-induced myocarditis is a big deal, and in children
it’s way more serious and more prominent than a post-COVID myocarditis.”
In addition to myocarditis, atrial fibrillation in young
people and pericarditis can also occur post-COVID-19 shot. The second category
of shot-induced syndromes is neurologic, which causes neurological symptoms
similar to those among COVID-19 long haulers, as well as additional, more
serious, effects. This includes Guillain-Barré syndrome, which can be fatal,
bell’s palsy, seizures, persistent headaches and blood clots in the brain.
The third category is immunologic, which includes
suppression of lymphocyte count and reactivation of other viral syndromes,
including Epstein-Barr virus and shingles. The fourth category — hematologic —
occurs about two weeks after the shot and describes vaccine-induced
thrombocytopenic purpura.
Signs include bruising all over the body, bleeding from the
gums and nose and dark urine. If you notice these signs in the weeks after receiving
a COVID-19 injection, get to a hospital immediately.
“What happens,” McCullough says, “is the [shot] tricks the
body and gives excessive antigenic presentation of platelets to the spleen, the
spleen produces an antibody that actually pins platelets against blood vessel
walls … and that’s what drives vaccine-induced thrombocytopenic purpura.”
For those suffering from these shot-induced syndromes,
FLCCC’s I-RECOVER20 protocol for long-haul COVID syndrome has been used to
treat shot-induced symptoms with similar success. The protocol can be
downloaded in full,21 giving you step-by-step instructions on how to treat
long-haul COVID syndrome and/or reactions from COVID-19 injections.
Sources and
References
- 1 CDC,
COVID-19, Post-COVID Conditions September 16, 2021
- 2 YouTube October 25, 2021
- 3 YouTube October 25,
2021, 5:43
- 4 Mayo
Clinic, COVID-19 Long-term effects
- 5 YouTube October 25,
2021, 6:04
- 6 YouTube October 25,
2021, 6:15
- 7 YouTube October 25,
2021, 6:51
- 8 Lab Tests Online,
D-dimer
- 9 YouTube October 25,
2021, 8:36
- 10 YouTube October 25,
2021, 15:19
- 11 YouTube October 25,
2021, 18:30
- 12 YouTube July 5, 2021
- 13 medRxiv
September 6, 2021
- 14 Forbes
January 27, 2021
- 15 CNS Neurosci Ther. 2019
Aug;25(8):815-823. doi: 10.1111/cns.13124. Epub 2019 Apr 11
- 16 YouTube October 25,
2021, 24:46
- 17 Neuroscience.
2003;120(1):113-20. doi: 10.1016/s0306-4522(03)00244-6
- 18, 20, 21 FLCCC
Alliance, I-RECOVER
- 19 YouTube October 25,
2021, 33:17
+
Blaylock’s COVID Vaccine Protocol
https://www.blaylockreport.com/
by
Dr. Russell Blaylock
Dr. Blaylock was not only known for being an
amazing neurosurgeon, he’s a lecturer, author, founder of Theoretical
Neuroscience Research, LLC and Associate Editor of the Neuroinflammation
section of Surgical Neurology International. (He also writes The Blaylock Wellness Report, which I highly recommend subscribing to.)
Dr. Blaylock has also become one of my very good friends and gave me permission
to share his COVID vaccine protocol with you. This post is not medical advice.
It is for information purposes only. Use (or don’t use) this protocol at your
own risk. If you want to keep your blinders on and pretend that these
quackxines have zero negative effects whatsoever on your body, you should stop
reading here. Otherwise, proceed to the protocol.
- 50 billion CFU of several acidophilus and
bifidobacterial strains — along with a GOS probiotic — each
morning before breakfast
- A B-complex
vitamin (Pure Encapsulation)
- Nano-vitamin C
500mg capsules (three between each meal)
- Buffered Vitamin C with Hepseridin —
three 500mg capsules with each meal.
- L-carnitine
500 mg three times a day with meals.
- NAD+ nicotinamide —
one capsule a day
- Nano-Curcumin —
two 250mg capsules with each meal
- Nano-Quercetin —
one 250mg capsules with each meal
- Nano-Bacopa —
two capsules twice a day with a meal
- NAC 900 mg capsules — two capsules taken with
a meal once a day.
- Mixed tocotrienols —
150 mg a day
- Magnesium citrate/malate
(Pure Encapsulation) a powder — 250mg dissolved in 4 ounces of water three
times a day
- Baicalin 250 mg dissolved in water (4 ounces)
twice a day
Note: This can be mixed with the magnesium, and is a powerful antiviral. - Pterostilbene —
200 mg twice a day with a meal.
- CoQ10 — 600mg taken three times a day with food
(Doctor’s Best)
- Astragalus —
one capsule a day (enhances lymphocyte production)
- Benfotiamine in
a dose of 150mg twice a day with a meal for brain protection.
- One adult aspirin for day if magnesium +
nanocurcumin are not available and an emergency “stop-gap” is needed.
For those unable to take pills, numbers 2, 4,
5, 7, 8, 12 and 13 can be dissolved in water and have very little taste when
mixed together.
Blaylock said the main effects of COVID
vaccines are centered around inflammation and macrophage/microglial activation.
“These supplements listed above powerfully inhibit these two processes,” he
said.
COVID vaccines also induce thrombosis (blood clots) and micro-thrombosis, thus
many of these supplements will slightly thin the blood and prevent blood clots,
such as the magnesium, nano-quercetin and nano-curcumin.
Blaylock said magnesium is the most important thing on the list, as it alters
the rheology of the red blood cells to reduce risks and also acts as a mild
anticoagulant, while vitamin C inhibits excessive coagulation.
“Hydration is also essential,” he said. “One
should drink at least five or six glasses of purified water a day. White tea
also inhibits the inflammation and suppresses many viruses.”
For conventional vaccines, Blaylock recommended using a cold pack on the
injection site to block the immune reaction. For COVID vaccines the opposite
may be true:
Heat may inactivate the nanolipid carrier and
destroy the mRNA, which is why they keep most of the vaccine in very cold
storage. Later, say days to weeks, it may be helpful to take very cold showers
or if available use the cold treatments at a special center, such as Core
Cryotherapy center. Cold blocks the immune reactions and could prevent the
damage that occurs later. IV vitamin C plus magnesium infusions would also help
reduce symptoms.
Dr. Blaylock said I was free to use his
protocol as I pleased, so I’m assuming the same applies to all of you. Good
luck!
Editor’s note: To locate these supplements, you will have to do your own
online search. (I had no issue finding them.) Ideally, you would be on this
protocol shortly before getting vaccinated, but if you already have been, it’s
better late than never. How long you should do the protocol depends on the person
-- age, weight, health issues, adverse events, vaccine etc. There’s no one-size
fits all. Some have done it for six months. Others have stayed on it longer.
Assess your own health, gauge your symptoms and use your best judgment.
______________________
|
Critiques of this
Vaccine Protocol. . . . https://meganredshaw.substack.com/p/covid-vaccine-protocol-what-to-do/comment/3273000 |
===========
k.
|
|

+
===========
l.
NIH and
EcoHealth Colluded to Evade Research Restrictions

https://www.youtube.com/watch?v=wwGVMA51xDo
Analysis by
Dr. Joseph Mercola Fact
Checked
Story
at-a-glance
- Emails
reveal the National Institutes of Health colluded with EcoHealth Alliance
to circumvent federal restrictions on gain-of-function (GOF) research and
avoid oversight
- NIH
officials allowed EcoHealth Alliance to craft oversight language governing
its own GOF experiments
- At
least two NIH officials expressed concern that the experiment might fall
under the designation of GOF banned under federal moratorium. They later
accepted EcoHealth’s illogical justification for why the research should
not be restricted
- The
NIH is now trying to evade responsibility by shifting blame for the
unlawful research onto EcoHealth Alliance, saying they violated the grant
rules
- According
to EcoHealth president Peter Daszak, the parent virus for his proposed
chimeric SARS-like viruses, WIV1, had “never been demonstrated to infect
humans.” Yet three months earlier, his collaborator, Ralph Baric, Ph.D.,
had published a paper showing WIV1 did indeed have the ability to infect
humans and posed a threat to the human population
The walls are closing in on Dr. Anthony Fauci as emails
reveal the National Institutes of Health colluded with EcoHealth Alliance to
circumvent federal restrictions on gain-of-function (GOF) research.
The damning revelations were published by The Intercept1 and Daily
Caller,2 November 3,
2021. While the NIH has kept the grant correspondence secret, only allowing
select congressional staff to review the documentation in a private session,
The Intercept was given access to their personal notes.
Considering federal grants are of clear public interest, the
NIH’s decision to not make the correspondence public is suspicious in and of
itself. Are they hiding something? You bet. As reported by Intercept
journalists Sharon Lerner and Mara Hvistendahl:3
“Emails show that NIH officials allowed EcoHealth Alliance
to craft oversight language governing its own gain-of-function research ...
Detailed notes on NIH communications obtained by The
Intercept show that beginning in May 2016, agency staff had an unusual exchange
with Peter Daszak, the head of EcoHealth Alliance, about experiments his group
was planning to conduct on coronaviruses under an NIH grant called
‘Understanding the Risk of Bat Coronavirus Emergence’4 ...
EcoHealth was entering the third year of the five-year, $3.1
million grant that included research with the Wuhan Institute of Virology and
other partners. In a 2016 progress report, the group described to NIH its plans
to carry out two planned experiments infecting humanized mice with hybrid
viruses, known as ‘chimeras.’
The plans triggered concerns at NIH. Two staff members —
Jenny Greer, a grants management specialist, and Erik Stemmy, a program officer
handling coronavirus research — wrote to EcoHealth Alliance to say that the
experiments ‘appear to involve research covered under the pause,’ referring to
a temporary moratorium5 on funding
for gain-of-function research that would be reasonably anticipated to make MERS
and SARS viruses more pathogenic or transmissible in mammals ...
Initially, NIH staff appeared intent on enforcing the
funding pause ... But what happened next sets off alarm bells for biosafety
advocates: Agency staff adopted language that EcoHealth Alliance crafted to
govern its own work.
The agency inserted several sentences into grant materials
describing immediate actions the group would take if the viruses they created
proved to become more transmissible or disease-causing as the result of the
experiments.”
NIH Tries to
Evade Responsibility
The NIH is now trying to evade responsibility by shifting
blame for the unlawful research onto EcoHealth Alliance. October 21, 2021, NIH
principal deputy director Lawrence Tabak, Ph.D., sent a letter6,7,8 to James
Comer, ranking member of the Committee on Oversight and Reform, “to provide
additional information and documents regarding NIH's grant to EcoHealth
Alliance Inc.”
In the letter, Tabak acknowledged that Fauci lied to
Congress when he emphatically insisted the NIH/NIAID have never funded GOF
research. However, when it comes to circumventing the research moratorium,
Tabak lays the blame squarely at the feet of EcoHealth. According to Tabak:9
“The limited experiment described in the final progress
report provided by EcoHealth Alliance was testing if spike proteins from
naturally occurring bat coronaviruses circulating in China were capable of
binding to the human ACE2 receptor in a mouse model ...
In this limited experiment, laboratory mice infected with
the SHC014 WIV 1 bat coronavirus became sicker than those infected with the
WIV1 bat coronavirus. As sometimes occurs in science, this was an unexpected
result of the research, as opposed to something that the researchers set out to
do ...
The research plan was reviewed by NIH in advance of funding,
and NIH determined that it did not to fit the definition of research involving
enhanced pathogens of pandemic potential (ePPP) because these bat coronaviruses
had not been shown to infect humans. As such, the research was not subject to
departmental review under the HHS P3CO Framework.
However, out of an abundance of caution and as an additional
layer of oversight, language was included in the terms and conditions of the
grant award to EcoHealth that outlined criteria for a secondary review, such as
a requirement that the grantee report immediately a one log increase in growth.
These measures would prompt a secondary review to determine
whether the research aims should be re-evaluated or new biosafety measures
should be enacted. EcoHealth failed to report this finding right away, as was
required by the terms of the grant.”
In other words, EcoHealth’s experiment “accidentally” turned
into GOF. At that point, EcoHealth should have alerted the NIH, but allegedly
didn’t. So, according to Tabak, NIH bears no responsibility as they relied on
EcoHealth to follow the terms of the grant.
EcoHealth has denied this charge, saying “These data were
reported as soon as we were made aware, in our year four report in April 2018
... At no time did program staff indicate to us that this work required further
clarification or secondary review.”10,11
As noted by The Intercept,12 Tabak
implies the NIH created that reporting rule “out of an abundance of caution,”
but according to the correspondence The Intercept reviewed, “the language was
inserted at Daszak’s suggestion,” and “the NIH and EcoHealth Alliance worked
together to evade additional oversight.”
Illogical
Justifications
How did they evade additional oversight? Through illogical
and contradictory risk assessments. While Tabak claims the resulting virulence
was unintentional, how could that be, since the experiment in question was
supposed to test the “emergency potential” of bat coronaviruses in the human
population?
The name of the grant itself tells us they’re going to
assess the possibility of a bat coronavirus mutating into something that can
affect humans, and to do that, they will likely try to manipulate the virus to
see if it can gain that function.
EcoHealth president, zoologist Peter Daszak, suggested to
the NIH that the experiment should not be categorized as restricted GOF because
his proposed hybrid viruses were so different from the SARS virus (which is
known to infect humans). The Intercept continues:13
“Daszak also pointed out that WIV1, the parent of the
proposed chimeric SARS-like viruses, ‘has never been demonstrated to infect
humans or cause human disease,’ according to the transcribed emails.
And he said that previous research ‘strongly suggests that
the chimeric bat spike/bat backbone viruses should not have enhanced
pathogenicity in animals.’ The NIH would go on to accept these arguments.
But the group’s argument that its viral research did not
pose a risk of infection appears to contradict the justification for the work:
that these pathogens could potentially cause a pandemic.
‘The entire rationale of EcoHealth’s grant renewal on
SARS-related CoVs is that viruses with spikes substantially (10-25%) diverged
from SARS-CoV-1 pose a pandemic risk,’ said [Fred Hutchinson Cancer Research
Center virologist, Jesse] Bloom.
‘Given that this is the entire rationale for the work, how
can they simultaneously argue these viruses should not be regulated as
potential pandemic pathogens?’”
But Daszak’s justification makes no sense for yet another
reason. Three months before Daszak wrote that determination for the NIH — where
he suggests the WIV1 virus they were going to use as the backbone for the
chimeras had “never been demonstrated to infect humans or cause human disease”
— his collaborator, Ralph Baric, Ph.D., had published a paper14 showing
WIV1 did indeed have the ability to infect humans.15
This is terrific! We are very happy to hear that our Gain of
Function research funding pause has been lifted. ~ Dr. Peter Daszak, email to
NIH
Baric, who works at UNC Chapel Hill, had found the WIV1
virus “readily replicated efficiently in human airway cultures and in vivo,”
and posed an “ongoing threat” to the human population. This completely contradicts
Daszak’s statement, and it’s doubtful that Daszak would not be aware of the
paper published by Baric three months earlier. It’s doubtful the NIH would be
ignorant of Baric’s finding as well.
NIH Accepted
Daszak’s Escape Clause
As explained by The Intercept, Daszak came up with a
solution that would allow his group and the NIH to perform research they all
knew was prohibited at the time:16
“If the recombinant viruses grew more quickly than the
original viruses on which they were based, [Daszak] suggested, EcoHealth
Alliance and its collaborators would immediately stop its research and inform
their NIAID program officer ...
In a July 7 letter to EcoHealth Alliance, NIH’s Greer and
Stemmy formally accepted Daszak’s proposed rule. The chimeric viruses were ‘not
reasonably anticipated’ to ‘have enhanced pathogenicity and/or transmissibility
in mammals via the respiratory route,’ the administrators concluded ...
The language that the NIH later inserted into the grant was
strikingly similar to what Daszak proposed: ‘Should any of the MERS-like or
SARS-like chimeras generated under this grant show evidence of enhanced virus
growth greater than 1 log over the parental backbone strain you must stop all
experiments with these viruses.’”
In a July 2016 email to the NIH, Daszak expresses his
satisfaction that the agency decided to accept his justifications for why the
research should not be considered restricted GOF. “This is terrific!” he wrote.
“We are very happy to hear that our Gain of Function research funding pause has
been lifted.”17 Daszak even admits that what they’re REALLY doing is GOF
right in that email.
Clear
Regulatory Failure
When EcoHealth’s scientists performed the experiment, one of
the chimeric viruses grew much faster than the others during the first week of
the experiment, producing a viral load that was four logs greater than the
parent virus.
As noted earlier, Tabak claims EcoHealth didn’t inform the
NIH program officer about this gain of function, and EcoHealth claims it did,
and was permitted by default to continue, as no one at the NIH objected.
Incidentally, Daszak was relying on Wuhan Institute of
Virology researcher Shi Zhengli — known to have ties to the Chinese military —
to notify him if any of the viruses in the experiment had enhanced replication.
Daszak in turn informed the NIH about this chain of reporting, so they knew the
legality of the research basically rested in the hands of a Chinese operative,
who may or may not have incentive to downplay such findings.
Richard Ebright, a molecular biologist at Rutgers University
who has criticized the lack of oversight of gain-of-function research, told The
Intercept that the correspondence between the NIH and EcoHealth points to clear
regulatory failure. “The oversight process clearly failed,” he said. Ebright
also spoke to the Daily Caller, stating:18
“The NIH, incredibly, accepted EcoHealth’s belief that this
work would not be considered gain of function, and accepted EcoHealth’s
rationale for this belief, and accepted EcoHealth’s policy-noncompliant
proposal for a [10 times] allowance for increased viral growth before stopping
work and reporting results.
The NIH, in effect, delegated to EcoHealth Alliance the
authority to determine whether its research was, or was not gain of function
research subject to the funding pause, the authority to set criteria for the
determination, and the authority to over-ride federal policies implemented by
the White House ...”
The same sentiment was expressed by House Energy and
Commerce Committee ranking member Rep. Cathy McMorris Rodgers and several other
Republican lawmakers in an October 27, 2021, letter19,20 to NIH
director Dr. Francis Collins. As reported by Daily Caller:21
“’EcoHealth portrayed the risks of these experiments as if
they were not of concern, and the NIH accepted EcoHealth’s assertions without a
searching inquiry,’ the Republican lawmakers told Collins. ‘However, the
assessment of the risks by both EcoHealth and the NIH do not seem to square
with the understanding of the research risks at that time ...
Although the engineered viruses at the WIV were far from
SARS CoV-2 on the coronavirus family tree, this research reflected a high
tolerance for risk,’ the lawmakers said, adding that there is no evidence that
EcoHealth took action to notify the NIH that it created viruses that exhibited
enhanced growth in humanized cells.
‘If EcoHealth and NIH could not handle compliance and
oversight of such a basic policy, it raises more concerns about the overall
adequacy of the oversight of this research, which leaves the public vulnerable
to a serious lab accident,’ the lawmakers wrote.”
CNN Grills
NIH Director
In a rare attempt at real journalism, CNN’s Pamela Brown
kept Collins strapped to the hot seat in a recent interview, repeatedly
grilling him about why the NIH was funding dangerous GOF research.22 Even Josh
Rogin from the liberal Washington Post picked up on Brown’s dogged demands for
Collins to come clean on the issue in the face of Collins’ attempts to
sidetrack her:
“Everyone should watch this interview with outgoing NIH
director Francis Collins to see how Collins uses misleading talking points to
avoid any acknowledgement NIH was caught completely unaware its grantee was
doing risky bat coronavirus research in Wuhan ... Collins uses every rhetoric
trick to dissemble and distract ...” Rogin tweeted.23
To her credit, Brown repeatedly brought the interview back
on track, pressing Collins for answers, demanding to know:
“Why should Americans trust you and the NIH on the issue of
COVID origins, when you didn’t even know about the programs it was funding with
taxpayer dollars in China?"
When Collins tried to circumvent the question by diving into
semantics about the definition of GOF, Brown interrupted him, again asking how
he can be so certain that NIH funding isn’t being used for GOF, when he claims
the NIH only recently found out about how the money was used in 2016?
Collins also reiterated that while EcoHealth “did some
things they should have told us about ... they did not do the kind of
gain-of-function research that requires special, high-level oversight.” Really?
As noted by ZeroHedge:24
“... if EcoHealth HAD reported its research results, it
WOULD HAVE triggered extra, high-level oversight. Why is Collins pretending he
knows they would have been exempt from that?”
Despite Collins’ insistence that the NIH was above-board and
honest in all its communications, Brown refused to let him off the hook, ending
the interview with: “This is U.S. taxpayer dollars going to risky research and
I believe every American deserves to know about it.”
On a sidenote, like Fauci’s, Collins’ halo is rapidly
tarnishing as alternative media have started digging into their backgrounds.
While appearing squeaky clean on the surface, a closer look reveals both men
have supported all sorts of questionable research, including research on
aborted fetuses.
For an overview of Collins’ alleged sins, see First Things’
article, “The Cautionary Tale of Francis Collins.”25 Unlike
Fauci, though, Collins seems to sense he won’t escape public judgment. In
October 2021, he announced his retirement from the NIH. He’s reportedly
planning to step down by the end of the year. Time will tell if Fauci will have
the good sense to resign, or if our political leaders will finally boot him out
and press charges.
We Must Ban
GOF Research
The evidence of regulatory failure by the NIH further
strengthens the call for a permanent ban on most kinds of GOF. As Bloom told
The Intercept:26
“We urgently need a broader discussion about whether it’s a
good idea to be making novel chimeras of coronaviruses that are at this point
universally acknowledged to pose a pandemic risk to humans.”
Indeed, it appears we got off easy this time. SARS-CoV-2 has
a very low mortality rate, despite spreading quite easily. The next Frankenstein
pathogen to escape from a lab might not be as benign.
Seeing how the people in charge of making decisions about
what research is to be allowed cannot be trusted with making sensible
decisions, the public really needs to step up and let our representatives know
we will not tolerate federal funds — taxpayer money — being used for research
that has the potential to wipe us all out.
Sources and
References
- 1, 3, 12, 13, 16, 26 The Intercept November 3, 2021
- 2, 15, 17, 18, 21 Daily Caller November 3,
2021 (Archived)
- 4 NIH Notice of Award, Understanding Risk of Bat
Coronavirus Emergence
- 5 PHE.gov US Gov. GoF Research Pause
- 6 Twitter Richard Ebright NIH Letter dated October 20,
2021
- 7, 9 NIH Letter dated October 20, 2021
- 8, 10 Vanity Fair October 22, 2021
- 11 ZeroHedge October 25, 2021
- 14 PNAS
March 15, 2016 113 (11) 3048-3053
- 19 Congressional Letter to Francis Collins October 27,
2021
- 20 E&C Republicans November 3, 2021
- 22, 24 ZeroHedge October 27, 2021
- 23 Twitter Josh Rogin October 25,
2021
- 25 First Things October 29, 2021
+
Fake News: How an ivermectin story got amplified around the world
when nobody seemed to check the facts
by Sharyl Attkisson
+
From:
Dragan Pavlovic
Sent: Saturday, November 20, 2021
Subject: Re: Legal history made in Alberta, Canada: Light at the end of the
tunnel?
Part I
“Selection Bias in the Covid-19 Clinical Studies”[1]
Retractions of The Lancet and The NEJM Hydroxychloroquine Papers
_______________________________________________________________
Dragan Pavlovic (corresponding author)
Adjunct
Professor of Anesthesiology
Department of Anesthesia, Pain Management and Perioperative Medicine
Dalhousie University, Halifax
QEII Health Sciences Centre
10 West Victoria, 1276 South Park Street
Halifax, NS B3H 2Y9 Canada
dragan.pavlovic@gmail.com
______________________________________________________________________
Abstract.
It was
claimed that a combination of hydroxychloroquine and azithromycin may have some
preventive effects for Covid-19 infection. Nevertheless, this has been
challenged between others by two large retrospective clinical studies, by a
group from Harvard Medical School, whose articles were published in The Lancet and the New England Journal of Medicine and then 10 days after, the
articles were retracted because of legal reasons. We claim no knowledge about
the efficacy of the hydroxychloroquine (HCQ) and do not discuss the
agent at all. However, here we claim that besides legal reasons, the
methodological reasons for the withdrawal of the papers were even more
important. The patients that receive HCQ during spring 2020. were predominantly
the high-risk patients and it was not possible to have a retrospective study
that would not suffer from selection bias. This means that the studies compared
incomparable groups and failed to demonstrate the link between the agent and
the outcome. The error is so flagrant that it is impossible that the
investigators, 3 highest medical authorities as well as and primarily The Lancet or NEJM reviewers, overlooked it. We proposed that even if correctly
performed, some eventual Randomised Controlled Trial ( RCT) will be very hard
to interpret because of always present potential various hidden errors and that
the conclusion of such studies should always be taken with much reserve.
Probably some more reliable methods of clinical research should be developed in
the future.
Keywords: hydroxychloroquine, chloroquine, Covid-19,
Randomised Controlled Trials, The Lancet, retracted article.
DOI:
10.35088/e4xq-1q16
____________________________________________________________________
Introduction
Clinical
research is a complex enterprise and methodological errors are hard to avoid.
Most often the researchers are not conscious of the errors that their otherwise
solid research projects contain. Even the journals of the highest reputation
will sometimes be victims of pressures to publish research papers that may have
hidden fundamental mistakes. This may particularly be the case if the issue is
important and the political and public pressures are high, as is the case now
with the Covid-19 pandemic since presently, there is no causal therapy for this
viral infection.
It was
claimed that a combination of hydroxychloroquine and azithromycin may have some
preventive effects for Covid-19 infection. Nevertheless, this has been
challenged between others by two large retrospective clinical studies, by a group
from Harvard Medical School, whose articles were published in The Lancet and the New England Journal of Medicine and then 10 days after, the
articles were retracted because of legal reasons. We claim no knowledge about
the efficacy of the hydroxychloroquine (HCQ) and do not discuss the
agent at all. However, here we claim that besides legal reasons, the
methodological reasons for the withdrawal of the papers were even more
important.
Below, we
will first give a shortlist of the problems and mistakes and then discuss just
the first cited paper initially published by The Lancet.1 The
third cited article, by Cavlacanty et al.2 has similar mistakes as
the first two and will not be analysed in detail. The paper of the Marseilles
group,3 that somehow initiated the debate, will be just cited but
not analysed. The three concerned papers, one from The Lancet and two from the NEJM,
are as follows (a, b, c):
- Mandeep R Mehra et al. Hydroxychloroquine
or chloroquine with or without a macrolide for treatment of COVID-19: a
multinational registry analysis1
- Mandeep R. Mehra et al. Cardiovascular
Disease, Drug Therapy, and Mortality in Covid-194
and
- Cavalcanti,
A. B. et al., Hydroxychloroquine with or without Azithromycin in
Mild-to-Moderate Covid-192
Our
Commentary on the first, The Lancet
paper, by Mehra et al,1 that we submitted on 23 May 2020 (corrected
in the following 2 days under the code: “THELANCET-D-20-11873”) was ignored by The Lancet. No reply to the second
appeal has been received.
The
researchers from the Harvard Medical School produced the above-mentioned papers
(2 first papers) in May 2020. Nine months after that scandal, I believe since
the spirits are calmed, we can look at the matter with more reason. We claim
that the articles, besides the probable absence of the facts and truths and
legal problems, (that we do not address), contained methodological mistakes.
The research that concerned HCQ therapy was in the focus of all media. The
controversy is nothing strange in science. Yet, the real problems, no doubt,
are those Harvard papers that were, methodologically, a failure. Harvard University is (or has been)
one of the top universities in the world. Besides, the papers were published in
the most valued "worldly" medical journals – and then retracted as
“almost” frauds. While the Marseilles paper3 that initiated the
debate, was a simple report on the use of a possible drug for the Covid-19
patients that urgently needed therapy, Тhe Lancet and the NEJM papers were scientific failures
combined with a major public scandal.
The following calendar of the events
will be useful to understand the problem:
13th January 2020, withdrawal of HCQ from the
pharmacies in France
End of March 2020, HCQ forbidden to be
used by the GPs
for the COVID-19 patients in France.
22nd May 2020, The Lancet paper appeared online.
23rd May 2020, HCQ was forbidden by the WHO and in
France to be used for COVID-19 outside of the specialised institutions.
Then,
on 2-3 July, the WHO forbids again the experimentation with HCQ - despite the
publication (one day before) of the Arshad et al. large Detroit study which
confirms certain (important) effects of the HCQ therapy.5
It is not easy to believe that just by
mistake (i) the Harvard scientists would conceive such a study, (ii) that the
two most prominent medical journals would accept to publish such papers, that
(iii) the World Health organisation (WHO), (iv) the French government and (v)
the French Scientific counsel would, one day after the publication of The Lancet paper, ban the use of the
HCQ.6 Where was the methodological problem?
Selection
bias and Covid-19 Therapy
The work
by Mehra et al.3 is an interesting analysis of a multinational
registry. However, first of all, the reader should be reminded that this
analysis is based on retrospective, historical data - a type of clinical
studies that have been known for years to contain many errors that not
randomized historical approach research may have. It looks like the analyses
that were often praxis in the fifties and sixties of the past century, often
based on retrospectively big collections of data that, unfortunately, produced
many unreliable conclusions. Particularly if they were multicentre and very
large studies. The problems with such studies are abundant and it will be
impossible to list even the most important. Indeed, we
will discuss here only The Lancet
paper methodology, restricting our discussion just to a small trivial
fraction of the methodological
problems. The legal questions have been communicated by several other
commentators directly to The Lancet
(the journal never disclosed them to the public) and they were such that the
authors retracted the two papers (the NEJM paper also) 10 days after
publication. Indeed we think that the methodological questions are of extreme
importance for the scientific community and should not be neglected. They are
indeed quite simple and visible to almost anyone.
The paper maintained, for example, that since non-survivals received
more often HCQ than survivals - HCQ was a cause of death of those patients. The
problem with such a conclusion is more than evident. An example with oxygen may
be sufficient. For example, the non-survivals had more often oxygen - why then
cannot the conclusion be that oxygen killed some COVID-19 patients? This would
certainly be confusing risk factors with causal factors, or even including
completely irrelevant factors. Or being over 65, obese, being in the ICU, would
be the risk factors but not causal factors. Similarly, a therapy that saves the
lives of some seriously ill patients cannot be confounded with causal factors
just because a majority of patients that die, receive such therapy, while the patients
that are not so gravely affected by the disease, survive “because they do not
have such a treatment”. This just sounds trivially false.
Furthermore,
how do we know that the control groups were comparable to the treatment groups?
The authors do not tell us this. In such a study it is very hard to
retrospectively fulfil the demands for fair randomisation. If more patients at
risk were in the group that was receiving HCQ and the healthier, not at-risk
patients, were in the control group, then the outcome would be heavily biased.
The tables show that the patients were similar (see the tables in the cited
paper), but do not show the degree of risks, which could be very different to
start with. One COPD is not the same as any other COPD. As looked at from the
outcome side, the non-survivals had much more often comorbidities than
survivals (Table 1, ref. 1), which implies a selection bias also.
So let us now look at the study from two sides, (A) before and (B) after
the event of disease and treatment and describe how this was done in reality.
A) How would it look from the start to the intervening physician? If we
assume normal behaviour of the physicians or just see how it was in France when
the government and the Scientific commission finally accepted to encourage
clinical studies, quite logically: the HCQ (that was withheld at first) had to
be administered only in hospitals and just to the patients at risk and with
more advanced serious symptoms. In fact, on March 24, 2020, HCQ was permitted
to be given only to patients with grave symptoms.7 The atmosphere in
France was against HCQ and for the use only in the patients with high risk (of
dying) - the agent was requisitioned by the governmental order already in
January 2020 for these purposes. The drug was not prescribed without bias
already from January 2020. The situation in the world was probably also
influenced by this "Zeitgeist".
Indeed, the Mehra et al. study1 included 50 European
hospitals, but the real question is: from which hospitals and how many patients
from France for example were included? A large number of Covid-19 patients in
France were to be included in the "Discovery" studies which should involve
over 800 hospitals only in France and should have included 3200 hospitals in
the world. These studies examined the mentioned agents only in patients at risk or gravely ill. If HCQ was given more to
patients that had more chances to die (what the regulation from 24. march, 2020
imposed) than for those that did not receive it, a selection bias was programmed. Besides, not to state in the study
how the hospitals and countries were chosen is a problem, since the number of
hospitals was large and the criteria of choice needed to be communicated and
the method about how the bias was avoided needed to be disclosed.
Also, the decision to administer or not the chloroquine or HCQ to the
patients presented with the Corona-19 symptoms (in the hospitals all over the
world - France included) was most probably spontaneously guided by the known
risk factors that the patients presented.
B) Let us then examine now how this looks like from the point of the
present time, retrospectively. No wonder, then, that we find, when we look
retrospectively, that more non-survivals received the mentioned HCQ therapy.
The finding that non-survivals have had the mentioned agent as therapy, was no
doubt, due to conscious, intelligent human intervention, a coherent behaviour
of the caring physicians or because the French physicians were obliged to
administer the agent only to the patients that had a higher risk of dying.
Also, it
seems that coronary artery disease, congestive heart failure, and arrhythmia
patients, received HCQ. Yet those were considered to be contraindications for
administrating the mentioned agents and can explain cardiac complications that
were observed in the study, in the groups that received those agents. The most
likely conclusion will then be that the agents produce undesirable
complications if used beyond the recommendations.
In
conclusion, this is again one in the series of non-randomized or in many
different ways problematic studies that try to evaluate the relevance of the
initial Marseille study.3 The Marseille study is
apparently in the middle or upper part of the low level on the Evidence-Based
Medicin Level scales8 so it is not to be rejected at this stage.
The analyses
of Mehra et al. and Cavalcanty et al., papers1,2 could only
demonstrate that the examined agents probably are not of much use for the
COVID-19 patients who are in the advanced phase of the disease and that if
used, the well-known contraindications should be respected. However,
we desperately need a study that verifies the initial Marseille finding,3
a coherent randomized clinical trial with the results that will contain hard
facts. Certainly, we should be aware that this will not be finally "a
clarification" but just a start of the efforts that will aim at finding
out whether HCQ may have some effects on COVID-19. The agent seems to have
antiviral properties in vitro9 and at least, for the respiratory
infections, apriori its use as aerosol may be envisaged preventively. We will
not elaborate more on this hypothesis here. What is needed is to establish
acceptable arguments in favour of its use, or its dismissal. Indeed,
the question that remains is what kind of randomised Clinical Trial (RCT) would
be able to establish a piece of reliable information. One different response is
urgently needed too: how the highest medical authorities (the World
Health Organisation [WHO)], the French government, the French Scientific
Commission) might have committed such a series of incoherent acts
in concert? Since this cannot be just an example of the “Swiss cheese model” of an accident,
there is little doubt that we had a serious, maybe even conscious,
methodological, scientific failure.
In the paper published in
2005, Ioannidis summarised some of the objections to the RCT that I discussed
above.10 A better approach may be a clear
pathophysiological method where we would rely on basic science and look for
mechanisms of the diseases and the mechanisms of action of the agents. The
principles of the RCT are wonderful, the principle of the "intention to
treat" is fine, but we need more. We need to know our patients better, The
method that we need should be the method that corresponds more to the subject
of the investigation that belongs somewhere in between pure science, medical science
and social science. We need to know the mechanisms of actions, cause-effect
relations, and the patients in all their sophistication. And before all, we
need morally fully justified methods, and we, certainly, need Reason.
Literature
1. Mehra, Mandeep R, Sapan S Desai, Frank
Ruschitzka, Amit N Patel, Hydroxychloroquine or chloroquine with or without a
macrolide for treatment of COVID-19: a multinational registry analysis, The Lancet, online of 23. May 2020,
https://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(20)31180-6.pdf (Viewed on
23rd May 2020); RETRACTED June 5, 2020:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31324-6/fulltext (Viewed on
June 5, 2020)
2. A.B. Cavalcanti, et al,
Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19, NEJM,
383; 21, 2020; 2041 – 2052.
This article was published online on
July 23, 2020, at the NEJM.
https://www.nejm.org/doi/pdf/10.1056/NEJMoa2019014?articleTools=true (Viewed on 23rd August 2020)
3. Gautret P, Lagier JC, Parola P, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results
of an open-label non-randomized clinical trial. Int J Antimicrob Agents
2020; 56, 1, 105949.
Published online March 20.
DOI:10.1016/j.ijantimicag.2020.105949. (Viewed on 23rd May 2020)
4. Mehra, Mandeep R., M.D., Sapan S. Desai,
M.D., PhD, SreyRam Kuy, M.D., M.H.S., Timothy D. Henry, M.D., and Amit N.
Patel, M.D. Cardiovascular Disease, Drug Therapy, and Mortality in Covid-19, NEJM, online, May 1, 2020,
https://www.nejm.org/doi/full/10.1056/NEJMoa2007621 (Viewed on
23rd August 2020)
RETRACTED June 5, 2020
https://www.nejm.org/doi/full/10.1056/NEJMc2021225?medium=organic-social&source=nejmtwitter; (Viewed
on 23rd August 2020)
5.
Arshad, Samia, Paul Kilgore, Zohra S. Chaudhry, et al.Treatment
with hydroxychloroquine, azithromycin, and combination in patients hospitalized
with COVID-19, Int J Infect Dis. 2020; 97:
396–403.
On line: https://www.ijidonline.com/article/S1201-9712(20)30534-8/fulltext (Viewed on 23rd August 2020)
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7330574/(Viewed on 23rd August 2020)
6. Matthias Blamont, Alistair Smout, Emilio Parodi, EU governments ban
malaria drug for COVID-19, trial paused as safety fears grow, Available:
https://www.reuters.com/article/us-health-coronavirus-hydroxychloroquine/france-bans-hydroxychloroquine-to-treat-covid-19-idUSKBN233197?il=0
(Viewed on 27th May 2020)
7. France allows
drug chloroquine to be given to gravest coronavirus cases, AFP,
24 March 2020.
https://www.thelocal.fr/20200324/france-allows-chloroquine-to-be-given-to-gravest-coronavirus-cases
(Viewed on 23rd May 2020)
8. From the Centre for Evidence-Based Medicine, Oxford.
For the
most up-to-date levels of evidence, see www.cebm.net/?o=1025.
Or, Stony Brok Univesity Library,
Frank Melville Jr., Memorial Library, Stony Brook University, Stony Brook, NY
11794-3300.
https://guides.library.stonybrook.edu/evidence-based-medicine/levels_of_evidence
(Viewed on 23rd May 2020)
9. Wang, Manli, Ruiyuan Cao, Leike Zhang, Xinglou
Yang, Jia Liu, Mingyue Xu, Zhengli Shi, Zhihong Hu, Wu Zhong and Gengfu Xiao, Remdesivir and chloroquine effectively inhibit the recently
emerged novel coronavirus (2019-nCoV) in vitro, Cell Research, 2020; 30:269–271;
https://doi.org/10.1038/s41422-020-0282-0.
10. Ioannidis JPA (2005) Why most published research findings are false.
PLoS Med 2(8): e124
*) Some important Internet sites,
viewed on 23rd May 2020:
Launch of a European clinical trial against COVID-19, Press release | 22 Mar 2020 - 13h00, INSERM PRESS OFFICE . Available:
https://presse.inserm.fr/en/launch-of-a-european-clinical-trial-against-covid-19/38737/
(Viewed on 23rd June 2020)
Arrêté du 13 janvier 2020 portant classement sur les
listes des substances vénéneuses
NOR :
SSAP2001007A
ELI : https://www.legifrance.gouv.fr/eli/arrete/2020/1/13/SSAP2001007A/jo/texte,
JORF n°0012 du 15 janvier 2020, Texte n° 13. Available :
https://www.legifrance.gouv.fr/jo_pdf.do?id=JORFTEXT000041400024
(The hydroxychloroquine is classified as a poisonous substance and practically
withdrawn from the pharmacies.) (Viewed on 23rd June 2020)
Benoît Zagdoun, Agnès Buzyn et son mari, Didier Raoult et la
chloroquine… On a examiné au microscope les 20 affirmations d'un message censé
prouver un "scandale d'Etat", Les allégations contenues
dans un message devenu viral sur les réseaux sociaux sont soit
fausses soit imprécises. Mais, surtout, elles ne prouvent rien. Franceinfo. Available :
https://www.francetvinfo.fr/sante/maladie/coronavirus/agnes-buzyn-et-son-mari-didier-raoult-et-la-chloroquine-on-a-examine-au-microscope-les-20-affirmations-d-un-message-cense-prouver-un-scandale-d-etat_3891385.html (Viewed on 23rd
June, 2020)
Décret n° 2020-314 du 25 mars 2020 complétant le
décret n° 2020-293 du 23 mars 2020 prescrivant les mesures générales
nécessaires pour faire face à l'épidémie de covid-19 dans le cadre de l'état
d'urgence sanitaire, Dernière mise à jour des données de ce texte : 26 mars
2020, NOR : SSAZ2008362D. Available :
https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000041755775&categorieLien=id (Viewed on
23rd June, 2020)
L’hydroxychloroquine n’est plus autorisée
en France pour traiter le Covid-19. La décision suit l’avis rendu
mardi par le Haut Conseil de la santé publique. Vendredi, une vaste étude
internationale concluait à un risque aggravé de mortalité chez les patients
atteints de Covid-19 traités avec ce médicament. Le Monde avec AFP. Publié
le 27 mai 2020 à 11h09 - Mis à jour le 27 mai 2020 à 13h54. Available :
https://www.lemonde.fr/sciences/article/2020/05/27/le-gouvernement-abroge-l-autorisation-de-l-hydroxychloroquine-pour-traiter-le-covid-19_6040915_1650684.html
(Viewed on 23rd June 2020)
Part II
“Facts or Values, that is
the Question”
Scientific and moral implications of The Lancet and the NEJM Hydroxychloroquine papers retractions.
_______________________________________________________________
Dragan Pavlovic (corresponding author)
Adjunct Professor of
Anesthesiology
Department of Anesthesia, Pain Management and
Perioperative Medicine
Dalhousie University, Halifax
QEII Health Sciences Centre
10 West Victoria, 1276 South Park Street
Halifax, NS B3H 2Y9 Canada
dragan.pavlovic@gmail.com
______________________________________________________________________
Abstract
The
search for some effective therapy of Covid-19 infection was marked at the very
beginning of the pandemic by an observational study where some positive effects
of the combination therapy with hydroxychloroquine and azithromycin were
reported. These results were challenged by at least two large, what was
presented as clinical studies from Harvard Medical School by Mehra et al. that
were published and then 10 days after retracted from The Lancet and the New
England Journal of Medicine. The studies contained serious errors: on the
one hand, illegal use of the patients' data and then, on the other hand, the
selection bias. Here we examined the various other sources of errors of
reasoning or possible technical difficulties linked to the Randomised
Controlled Trial (RCT) protocols executions, and some more fundamental
theoretical problems of reasoning, like vulgar contextualism. We proposed that
the RCT impose the confrontation of the facts with values which could be caused
by some errors of logic and that the results of such studies should always be
taken with much reserve and that probably some more reliable methods of
clinical research should be developed.
Keywords: hydroxychloroquine, chloroquine, Covid-19,
Randomised Controlled Trials, The Lancet, retracted article.
____________________________________________________________________
Introduction
Clinical
research is a complex enterprise and several methodological errors are hard to
avoid. Most often the researchers are not conscious of the errors that their
otherwise solid research projects contain. Sometimes the journals of the
highest reputation will be victims of pressures to publish solid research
papers that may have hidden fundamental mistakes. This may particularly be the
case if the issue is important and the political and public pressures are high,
as is the case now with the Covid-19 pandemic.
The
Harvard Medical School produced two important papers in May 2020 that claimed
that controversial therapy for Covid-19, hydroxychloroquine (HCQ) was not only
ineffective but dangerous1, 2. After about 10 days, the papers were
quickly retracted and HCQ was banned in many countries. We still do not have a
definitive answer to that dispute. The controversy is nothing strange in
science. Yet, the real problems, no doubt, are the consequences of those
Harvard papers that were, methodologically, a failure. Harvard University is (or has been) one of the top universities
in the world. Yet, in addition, the papers were published in the most valued
"worldly" medical journals – and then retracted as “almost” frauds.
While the Marseilles paper3 that initiated the debate, was a simple
report on the use of a possible drug for the Covid-19 patients that urgently
needed therapy, Тhe Lancet and NEJM papers were scientific failures
combined with a major public scandal (5 highest state health institutions
taking inconsequent actions). The study contained serious errors, on the one
hand, illegal use of the patients' data and then, on the other hand, the
selection bias.
The analyses
of Mehra et al. and Cavalcanty et al., papers1,3 demonstrate that
the examined agents probably are not of much use for the COVID-19 patients who
are in the advanced phase of the disease and that if used, the well-known
contraindications should be respected. However, we desperately
need a study that verifies the initial Marseille finding,4 a
coherent randomized clinical trial (RCT) with the results that will contain
hard facts. Certainly, we should be aware that this will not be finally "a
clarification" but just a start of the efforts that will aim at finding
out whether HCQ may have some effects on COVID-19. The agent seems to have
antiviral properties in vitro5 and at least, for the respiratory
infections, apriori its use as aerosol may be envisaged preventively. We will
not elaborate more on this hypothesis here. What is needed is to establish
acceptable arguments in favour of its use, or its dismissal. Indeed,
the question that remains is what kind of RCT would be able to offer a piece of
reliable information. One different response is urgently needed too: how 5
scientific, state and international institutions might have committed such a
series of incoherent acts in concert?
Vulgar Contextualism
The
problem of scientific misconduct and the evaluation of the scientific work may
be linked with fallacious reasoning. It has become popular to abandon classical
reasoning that employs formal logic and to apply various sorts of advanced
forms of reasoning that can be described by informal logic6
(intensional logic in particular). While the formal logic concerned
manipulation with the arguments without assigning meanings to the symbols that
formally represent the arguments, informal logic is supposed to pay attention
to the specific meaning of the arguments represented by a variety of logical
symbols and depends not only on the formal aspects of the arguments but much
more on the truth values of the facts, on how the world is, time, place, a
relation of the facts and other similar aspects. Therefore, in informal logic
attention is paid to the two aspects of the terms, at the families of the
aspects of the terms like sense/reference7 (that are Sinn/Bedeutung
in Frege), intension/extension, and connotation/denotation. In general the
first would stand for the meaning of the term while the second would concern
the range of the items to which the term applies8 (p. 21, ref 12).
The concept of intension would refer here to the meaning of the terms and not
the intentionality of consciousness (written with “t”).9
The
evaluation of scientific text is often linked to some theoretical reflection
about truth, beliefs, and meanings of the empirical evidence and the way of
presenting and evaluating their cognitive values. There are contexts, which may
be mutually exclusive and incompatible. Besides in some context, it appears
that truth and falsehood are losing their formal independent meaning. Some
global context can be accepted or rejected and therefore declared to be true or
false, but the truth values of some entities that are inherent in these
contexts are taken to be epistemically irrelevant and are overdetermined by the
normative definitions of the context to which they belong, irrespective of
their isolated meanings and character. This may lead to some absurdities, of
course. One of the most important applications of the method of Popper’s method
of piecemeal social engineering14 that
refers to the individual entities, i.e, that their cognitive value can be
viewed to great extent in isolation from the context can resolve the mentioned
absurdities and such an approach would remove some grave mistakes which are due
to the pernicious effects of the assumed context.
In
everyday life, we are obliged to base our actions on belief, not knowledge,
because knowledge is not available to us in new situations, and operational
conditioning has a delayed effect and requires a chain of reinforcing
mechanisms.10 Also, we cannot count on estimates based on the
probability of an outcome that would allow for perhaps adequate but belated
actions. Belief, in turn, relies on experiences related to the “typical
contexts” of global conditions10 (p.
50) for which we already have typical answers. The problem is that global
conditions, these typical contexts, are also beliefs.
Yet, in such
circumstances, blind mixing formal and informal logic reasoning may, as said,
produce absurdities. We know that the meanings of some propositions are
context-dependent, i.e. that their truth value depends on the context, like
various aspects of the situation, time, place and maybe some other conditions.
Such propositions or sentences need informal logical semantics where the
meanings are derived from the intension and extension or the conceptual content
of the proposition. This exemplifies the intention or in the other words, sense
(Sinn), where the conceptual context itself is the extension, or reference
(Bedeutung). Obviously, the propositions may have different extensions in
different contexts. As stated in the terms of the intensional logic, such
sentences may have multiple references (Bedeutung), i.e. as stated above,
multiple extensions. The sentences that we normally use in science are
content-independent, could be expressed by the traditional logic and are not
the subjects of intensional logic. In fact, the aim of the scientific method is
exactly this: to make the propositions of science context neutral. Certainly,
knowing how our concepts are in the real world is important, but this is
another aspect that is relevant but of a different nature.11
The fallacy employed in
the above mentions studies was in strong tendencies to make it
content-dependent what transformed the meanings of its propositions to be
strongly content-dependent too, which had repercussions on the meanings of the
very facts that were contained in the propositions. Concretely, in the present
studies, the obvious fact that the method of the study did not eliminate the
selection bias was taken to be irrelevant. Or it was taken that, contrary to
the clear evidence demonstrated in some empirical studies about the effects of
some agents on Covid-19, for example, the preventive effects of HCQ, it was
also taken to be spurious and irrelevant. On the contrary, the studies with the
mentioned selection bias were taken to be relevant. The context of the
predominant opinions was taken to be detrimental for the meanings of the
experimental or historical clinical trial findings. This introduced rare
scientific fallacy, rare at least in the natural sciences.
Such fallacies are
difficult to avoid in social sciences and have large implications in politics
and other social sciences in principle.12 Such approach will
sometimes lead the postmodernist interpreters of social events and social
theories to catastrophic conclusions: that everything is relative, that there
is no truth, no morals, no justice and that facts have no value of truth but
that the context is sufficient to determine the truth values. The belated
interpreters of these theories forget that such conclusions still basically
belong only to a specific context as well - to whom this theory belongs, and
that they cannot be literally translated outside their contextual framework.
All the mentioned conclusions may be completely wrong and the result will be an
unauthorized departure from the very context of the mentioned theories.13
I do not hide my conviction that I believe that the various aspects of the
crisis of today's world (social, moral, political (yet not the subjects of this
paper) are the direct result of the above-mentioned pernicious way of thinking,
"enriched", in the central and leading political circles, by a
favourite utilitarian logic.14, 15, 16, 17 This way of thinking makes the journals, especially
those from the social sciences, have their own specific publishing
"worlds". This makes it almost impossible to publish something in a
group of journals that differs in terms of macro concepts from the concepts to
which the text submitted to the press belongs - if they are different. The authors
are thus divided into groups belonging to special, clearly differentiated clans
that do not mix.
The
problems then multiply. Such an approach has further consquences leading to the
view that the improvement of society cannot be achieved by improving and
correcting individual facts and by small improvements, but that only global
changes lead to progress. It was not only the French Revolution that spread
such beliefs, but also Marxism or postmodernism; the same, only in a slightly
altered form we still have it on many micro-levels. And that is absurd. And the
root of that resides, for the most part, whether we like it or not, in our
scientific misconceptions. This belief was resisted by Karl Popper.18
Discussing the need for social change, the Austrian philosopher argued that the
general improvement of society (meaning social justice) is achieved by small
advances, a gradual grain-by-grain technique of piecemeal social engineering.19
In
our case, just withdrawing the first two articles from The Lancet and the NEJM
suggests no doubt about the piecemeal social engineering methodology at work.
Unfortunately, the behaviour of the World Health Organization, the response of
the French government and the highest medical bodies in France, points at the
strong influence of context on the decisions made and the neglect of the
meaning of the facts themselves.
Randomised Controlled Trials
(RCT) - an illusion of certainty
Scientific theories are ephemeral20, 21, as was maintained by
the philosophers Karl Popper and Thomas Kuhn. To illustrate this, let us first
list some very well known examples from the history of medical therapy. Low dose hydrocortisone in septic
shock was mandatory, it is not any more; Albumin was prohibited in sepsis, now
it is recommended; HAES (hydroxyethyl starch) was good as a volume replacement
in sepsis, now it is prohibited; intensified insulin therapy (initially
proposed by van den Berghe) was highly recommended; it is not any more; every
ICU patient had to regularly have Bisolvon (expectorant) in the past -
certainly no more. Cimetidine and Ranitidine until recently were administered
without exception to such patients; not any more. We gave APC (activated
protein C) to the septic patients 10 years ago - now no more. Or just remember
what was the cardio-pulmonary resuscitation protocol 30 years ago. Do you
remember bicarbonate or the frequency of lung inflation? Many therapeutical
measures were fundamentally changed, some methods banned. Therapy is verified
again and again in clinical trials and then either accepted, some therapy
modified, some rejected and even prohibited. Often, the corrections happen in
the form of retraction.22,23
Many
articles are “retracted” silently, over time the scientific community replaces
some agents, withdraw them from use or they are not recommended any more or
prohibited. Most of the time without any particular publicity. Science has its
history, knowledge increases, some old concepts are corrected, abandoned and
newly introduced. Some knowledge of today will be the ignorance of tomorrow.
What is then the value of a clinical study in principle and in the long run? We
do not know. The example of the above-mentioned problems is useful to look a
bit deeper into the problem of knowledge and particularly the methodology of
clinical research.
"Why on Earth Dr Raoult did not do one RCT, this was so simple.
Why?" was one of the frequently repeated objections to the Marseilles
group and their paper mentioned above. Some journalists and several reputed
professors of medicine insist on (sic) "one RCT about HCQ" that would
"solve" the controversy of that agent (HCQ) and, as a result of such
a study, Professor Raoult would be saved from the attacks and receive maybe the
Nobel prize... or proved to be wrong and his therapy banned. This was advanced
by the media repeatedly. Yet this is, I think, sadly a clear sign of ignorance.
The RCT do not in principle verify whether the agent by itself has some effect
on a particular disease. As we tried to show,16 such studies
establish only whether the particular therapy in some social settings
(hospital, outpatient, or any other well-determined settings) produces some
effect that is different from the effects of placebo. An ideal setting, that
would be at the same time of the investigation and therapy, the same place,
identical groups, identical all confounding factors, is impossible to arrange.
Clinical studies than in fact establish - together with the effects of the
examined agents, the effects of more than tens of more reasonably well or less
well-controlled factors, but including also several uncontrolled factors. The
result is often hard to interpret if the real differences of the presumed
effects are small. Even worse. If the differences found between groups are very
small, they may be accidental, despite coherent statistics. Often such studies
are organised in many medical centres where the conditions (that include human
and objective factors), from recruitment until therapy are so varied that no
homogeneity of the conditions is ever to be aspired to. Enormous efforts are
made to make clinical research as objective as possible but controversies
persist.24 As we could see, for example in the
Cavlacanty et al. study3 it has apart from the above-mentioned
shortcomings, other mistakes like late admission, various selection bias
versions, the exclusion of the patients that had previously HCQ or
Azithromycin, and the mentioned intention
to treat protocols.
Some other objections to the RCT are however fatal. One trivial but
serious is that if series of RTCs are undertaken to find the existence of the
effects of some agent, even if the agent has no effect, it is probable that
just one of 10 or more studies will show differences just by accident. This is
why the studies are supposed to be registered before they will be undertaken.
This is however not respected everywhere. More deep problems are linked to what
we said above. The fact that the set conditions, criteria, measurements of
different studies cannot be in principle completely standardised, the studies
cannot be compared one with another with sufficient confidence. The mentioned
conditions change with time also, comparison with the earlier studies is hard
if not impossible. It will not help if the methods of the studies are described
in all details. Several sets of conditions would differ anyway, and the
undeclared conditions, which certainly introduce further variations of unknown
factors, always accompany such large studies.
Finally, even if one such study would establish efficacy or no efficacy
of for example the HCQ for therapy for Covid-19, we will need a next study to
confirm the initial results, and this will not stop there. And we are on the
way to an infinite regress. So we will never be satisfied. When we know the
history of science and medicine and are aware that probably 30% of the results
of the studies, after about 30 years, are considered invalid and some agents
often even considered as contraindicated, we must conclude that to look for
some better methods (the more complex RTC?) is necessary. Besides, one other
“demon” disturbs us too: the moral problem25 of not treating the
sick patients in the control groups in the RCT has been lurking around for many
years now and we have just to wait for it to emerge with devastating effects
since it is simply insurmountable.
The
future
In the paper published in
2005, Ioannidis summarised some of the objections to the RCT that I discussed
above.26 The conditions that will render the results less likely,
i.e. the research findings to be true, after Ioannidis, would be: The small
studies; small effect size; the greater the number and the lesser the selection
of tested relationships; the greater the flexibility in designs, definitions,
outcomes, and analytical modes; On the contrary, the greater the financial and
other interests and prejudices, and the hotter a scientific field (with more
scientific teams involved), more chances will be to miss the important issues
and fail.
A better approach may be a clear pathophysiological method where we
would rely on basic science and look for mechanisms of the diseases and the
mechanisms of action of the agents. The method that we need should be the
method that corresponds more to the subject of the investigation that belongs
somewhere in between pure science, medical science and social science. We need
to know the mechanisms of actions, cause-effect relations, and the patients in
all their sophistication. And before all, we need morally fully justified
methods, and we, certainly, need Reason.
Literature
1. Mehra, Mandeep R, Sapan S Desai, Frank
Ruschitzka, Amit N Patel, Hydroxychloroquine or chloroquine with or without a
macrolide for treatment of COVID-19: a multinational registry analysis, The Lancet, online of 23. May 2020,
https://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(20)31180-6.pdf (Viewed on
23rd May 2020); RETRACTED June 5, 2020:
https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(20)31324-6/fulltext (Viewed on
June 5, 2020)
2. Mehra, Mandeep R., M.D., Sapan S. Desai,
M.D., PhD, SreyRam Kuy, M.D., M.H.S., Timothy D. Henry, M.D., and Amit N.
Patel, M.D. Cardiovascular Disease, Drug Therapy, and Mortality in Covid-19, NEJM, online, May 1, 2020,
https://www.nejm.org/doi/full/10.1056/NEJMoa2007621 (Viewed on
23rd August 2020)
RETRACTED June 5, 2020
https://www.nejm.org/doi/full/10.1056/NEJMc2021225?medium=organic-social&source=nejmtwitter; (Viewed
on 23rd August 2020)
3. A.B. Cavalcanti, et al,
Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid-19, NEJM,
383; 21, 2020; 2041 – 2052.
This article was published online on
July 23, 2020, at the NEJM.
https://www.nejm.org/doi/pdf/10.1056/NEJMoa2019014?articleTools=true (Viewed on 23rd August 2020)
4. Gautret P, Lagier JC, Parola P, et al. Hydroxychloroquine and azithromycin as a treatment of COVID-19: results
of an open-label non-randomized clinical trial. Int J Antimicrob Agents
2020; 56, 1, 105949.
Published online March 20.
DOI:10.1016/j.ijantimicag.2020.105949. (Viewed on 23rd May 2020)
5. Wang, Manli, Ruiyuan Cao, Leike Zhang, Xinglou
Yang, Jia Liu, Mingyue Xu, Zhengli Shi, Zhihong Hu, Wu Zhong and Gengfu Xiao, Remdesivir and chloroquine effectively inhibit the recently
emerged novel coronavirus (2019-nCoV) in vitro, Cell Research, 2020; 30:269–271;
https://doi.org/10.1038/s41422-020-0282-0.
6.
Gilbert Ryle, The theory of meaning, in: Caton CE (ed), Philosophy and ordinary language, Urbana, University of Ilinois
Press, 1963. p 128 and later.
7. Gottlob
Frege, Begriffsschrift, eine der arithmetischen
nachgebildete Formelsprache des reinen Denkens, Halle a. S.,
1789.
8. Anthony Grayling, An
Introduction to Philosophical Logic, Blackwell
Publishing, (1982), 1998, chapter 2.
9. Brentano,
F., , Psychology from an Empirical
Standpoint, London: Routledge and Kegan Paul. (1874,
1911), 1973.
10. Robert Nozick, The
Nature of Rationality, Prиnсtone University Press, 1993,
93-100.
11. Dragan Pavlovic. Two problems of empirical biomedical science:
example of awareness monitoring with bispectral analysis. Eur J Anesth, 2009; 26: 87-9.
12. Richard
Dawkins, Postmodernism
Disrobed, Nature 1998; 394:141–143.
13. Alan
Sokal et Jean Bricmont, Impostures intellectuelles, Éditions Odile Jacob, 1997.
14. Dragan Pavlovic, Christian Lehmann, Michael Wendt, For
an indeterminist ethics. The emptiness of the rule in dubio pro vita and life cessation decisions, Philos Ethics Humanit Med. 4(1), 6. http://www.peh-med.com/content/pdf/1747-5341-4-6.pdf (viewed 3. 6. 2018).
15. Bernard Williams, Utilitarianism: For and Against Edited
by: Smart JJ, Bernard Williams. Cambridge University Press; 1973.
16. John Rawls, A Theory of justice, Oxford University
Press; (1972) 1973, p. 170 and 320―325.
17. John Rawls, Political liberalism, Columbia
University Press, New York; 1993, p. 162.
18. Karl Popper, The
myte of the fraimwork, Routledge. 1994 (chapter 2 treats the ftaimwork, chapter 3 piecemiel engeniring).
19. Karl Popper, Open society and its enemies, (Routledge 1996) (1945), book 1,
chapter 9 notes for this chapter). Karl Popper, The povery of historicism, (1957) Routledge 1991; 3, 21.
20. Popper Karl, Conjectures and
Refutations, Harper and Row, 1968, ch 10.
21. Kuhn, Thomas, The structure of
scientific revolutions, University of Chicago Press, 1962.
22.
Famous retractions. Available:
https://retractionwatch.com/the-retraction-watch-leaderboard/top-10-most-highly-cited-retracted-papers/
23.
Top retractions in 2019, available: https://www.the-scientist.com/news-opinion/the-top-retractions-of-2019-66852
24.
Vincent, Jean-Louis, We should abandon randomized controlled trials in the intensive care unit,
Critical Care Medicine: 2010; 38, 10: S534-S538.
25.
Louhiala P., The ethics of the placebo in clinical practise revisited, J Med
Ethics, 2009; 35: 407-409.
26. Ioannidis JPA (2005) Why most published research findings are false.
PLoS Med 2(8): e124
*) Some important Internet sites,
viewed on 23rd May 2020:
Launch of a European clinical trial against COVID-19, Press release | 22 Mar 2020 - 13h00, INSERM PRESS OFFICE. Available:
https://presse.inserm.fr/en/launch-of-a-european-clinical-trial-against-covid-19/38737/
(Viewed on 23rd June 2020)
Arrêté du 13 janvier 2020 portant classement sur les
listes des substances vénéneuses
NOR :
SSAP2001007A
ELI : https://www.legifrance.gouv.fr/eli/arrete/2020/1/13/SSAP2001007A/jo/texte,
JORF n°0012 du 15 janvier 2020, Texte n° 13. Available :
https://www.legifrance.gouv.fr/jo_pdf.do?id=JORFTEXT000041400024
(The hydroxychloroquine is classified as a poisonous substance and practically
withdrawn from the pharmacies.) (Viewed on 23rd June 2020)
Benoît Zagdoun, Agnès Buzyn et son mari, Didier Raoult et la
chloroquine… On a examiné au microscope les 20 affirmations d'un message censé
prouver un "scandale d'Etat", Les allégations contenues
dans un message devenu viral sur les réseaux sociaux sont soit
fausses soit imprécises. Mais, surtout, elles ne prouvent rien. Franceinfo. Available :
https://www.francetvinfo.fr/sante/maladie/coronavirus/agnes-buzyn-et-son-mari-didier-raoult-et-la-chloroquine-on-a-examine-au-microscope-les-20-affirmations-d-un-message-cense-prouver-un-scandale-d-etat_3891385.html (Viewed on 23rd
June, 2020)
Décret n° 2020-314 du 25 mars 2020 complétant le
décret n° 2020-293 du 23 mars 2020 prescrivant les mesures générales
nécessaires pour faire face à l'épidémie de covid-19 dans le cadre de l'état
d'urgence sanitaire, Dernière mise à jour des données de ce texte : 26 mars
2020, NOR : SSAZ2008362D. Available :
https://www.legifrance.gouv.fr/affichTexte.do?cidTexte=JORFTEXT000041755775&categorieLien=id (Viewed on
23rd June, 2020)
L’hydroxychloroquine n’est plus autorisée
en France pour traiter le Covid-19. La décision suit l’avis rendu
mardi par le Haut Conseil de la santé publique. Vendredi, une vaste étude
internationale concluait à un risque aggravé de mortalité chez les patients
atteints de Covid-19 traités avec ce médicament. Le Monde avec AFP. Publié
le 27 mai 2020 à 11h09 - Mis à jour le 27 mai 2020 à 13h54. Available :
https://www.lemonde.fr/sciences/article/2020/05/27/le-gouvernement-abroge-l-autorisation-de-l-hydroxychloroquine-pour-traiter-le-covid-19_6040915_1650684.html
(Viewed on 23rd June 2020)
+
COVID
Shots Are the Deadliest ‘Vaccines’ in Medical History
analysis by Dr. Joseph
Mercola Fact Checked
(1:37:33)
Story
at-a-glance
- Data
suggest 1 in 317 boys aged 16 to 17 will get myocarditis from the COVID
shots, and after a third booster, that number may be even higher
- VAERS
reporting is likely underreported by a factor of 41. Since there are over
8,000 domestic deaths reported to VAERS, and 98% of those deaths are
“excess deaths,” this suggests that as many as 300,000 Americans may have
died from the COVID shots thus far
- Calculations
based on government data from 35% of the world’s population suggest we’re
killing approximately 411 people per million doses on average. Moderna and
Pfizer are both two-dose regimens, which pushes this to 822 deaths per
million fully vaccinated. And that’s just the short-term mortality. We
still have no concept of how these shots might impact mortality and
morbidity in the longer term
- An
Italian investigation found that if the COVID mortality definition were
changed to only include those cases where there were no preexisting
comorbidities, the mortality from COVID comes out to just 2.9% of the
overall reported number. This suggests that if a COVID death was redefined
to being a death actually “from” COVID rather than “with” COVID, the death
count could be substantially smaller than 760,000 deaths and may be
smaller than the number killed by the vaccines
- The
deadliest vaccine ever made is the smallpox vaccine, which killed 1 in 1
million vaccinated people. The COVID shots kills 822 per million fully
vaccinated, making it more than 800 times deadlier than the deadliest
vaccine in human history
In this interview, Steve Kirsch, executive director of
the COVID-19 Early Treatment Fund, reviews some of the COVID jab data he’s
presented to the U.S. Food and Drug Administration and the Centers for Disease
Control and Prevention during various meetings.
For example, during the September 17, 2021, FDA VRBPAC
(Vaccines and Related Biological Products Advisory Committee) meeting,1
Kirsch cited data suggesting 1 in 317 boys aged 16 to 17 will get myocarditis
from the shots, and after a third booster, that number may be even higher. He
also cited data showing the Pfizer shot kills far more people than it saves.
I’ll provide more details about that below.
Kirsch didn’t come into this due to some preconceived
opinion about vaccines. He and his family have all received two doses of the
COVID jab. It wasn’t until after the fact that he started hearing about
problems from others that he started taking deep dives into the data. He
explains:
“After I got vaccinated, a
woman asked me, ‘Should I get vaccinated?’ And I said, ‘Of course, you should.
This is the safest thing ever. Nobody's died and there are no side effects.
You've got to get this modern technology.’ I'm singing from the hymn book.
And then she said something
that threw me off course because I said, ‘Why are you asking such a stupid
question?’ And she said, ‘Well, three of my relatives got the vaccine and they
died within a week.’ I said, ‘No, no, that can't be true. There's no way that
can happen.’
I'm trying to convince her
that she's mistaken, that it must have been something else. I wrote her saying,
‘Statistically, you can't have three people dying from the vaccine, which
doesn't kill anyone.’ And she wrote back and she said, ‘Yeah, but they're
dead.’
That was a game-changing
moment for me ... but I was still in denial ... I was operating [from the
position] that the FDA is still operating the same [conservative] way [they
used to before], but they're not ... nor did I understand that the U.S. Centers
for Disease Control and Prevention is now mission driven, and the mission is to
get a needle in every arm. My trust was in the agencies.
The next incident involved my
carpet cleaner, Tim Damroth. He showed up wearing a mask. And I'm saying, ‘Hey,
you should all get vaccinated. Once you get vaccinated you don't have to wear a
mask.’ And he said, ‘Well, I did get vaccinated, but I had an extreme reaction.
I had a heart attack two minutes after I got injected.’ He also described that
his wife had [developed] Parkinson's-like symptoms. Her left hand was shaking
uncontrollably.”
The Price Truth-Tellers Pay
The data are ultimately what convinced him that people
must be told the truth about these shots because, without that, they cannot
give informed consent. He’s sacrificed a lot to do just that, including
professional relationships and millions of dollars in lost income.
“I basically put my life on
hold and started looking in the various databases and talking to people to
understand what was going on,” Kirsch says. “And every place I looked, [the truth] became more clear to me. And so,
on May 25, 2021, I wrote this 250-page article for TrialSiteNews. It may be the
longest article for TrialSiteNews ever published.
When I wrote that article,
within a week, every member of my [COVID-19 Early Treatment Fund’s] scientific
advisory board quit — there were 14 scientists from all over the United States
and in different fields with different expertise. They said I was ‘an evil
person’ and that they never wanted to talk to me again in their life.
I pleaded with them, saying,
‘Look, if I've got the analysis wrong, then tell why can’t you tell me where I
got it wrong.’ And they wouldn't say anything. They just said, the vaccines are
safe and I should be ashamed of myself.”
Kirsch also created and submitted a 177-page PDF
slideshow to the October 26, 2021, VRBPAC hearing, titled, “Questions
About the COVID Vaccine.”2
It’s an absolute treasure trove of information and I would encourage you to
review this great resource that he is updating in real time.
VAERS Data Likely Off by Factor of 41
In his video, “Vaccine Secrets: COVID Crisis,”3 the
first episode of “The False Narrative Takedown Series,” Kirsch explains how to
estimate COVID jab mortality, which he and a team of statisticians have done
based on a variety of sources, including but not limited to the U.S. Vaccine
Adverse Events Reporting System (VAERS).
Kirsch estimates VAERS reporting is off by a factor of
41, and that anywhere from 150,000 to 300,000 Americans have died from the
COVID shots.
“We looked at eight different
ways and VAERS is just one of the ways. So, when people say, ‘You can't use
VAERS for this, you can't [calculate] causality [based on VAERS data], I'm
saying, ‘Fine. We got the same answer using seven other ways.
In the VAERS analysis, we
determined that VAERS was under-reported by a factor of 41, which is quite
reasonable ... Ten years ago we had a system where we could actually discover
all the unreported things in VAERS, and they discovered VAERS was severely
underreported by as much as 95 times. Vaccines that we thought were safe,
they're not safe at all. So, what did they do? They killed the project.
So, the reason that we have
such a bad system today is that it is intentional. If we had a good system, it
would show all the flaws for all of these vaccines that we've been giving
people.”
The system is clearly intentionally designed from a technical
standpoint to radically decrease the number of cases entered. It takes more
than 30 minutes to complete a single report and you can’t save it until
completed, so if you walk away and get timed-out, you have to start all over.
Kirsch knows a neurologist in California who claims to
have 2,000 COVID jab-injured patients (out of a client base of 20,000), but
she’s only filed two reports to VAERS. She doesn’t have time for the rest. So,
she’s under-reporting by a factor of 1,000. Also, while doctors are required by
law to file adverse event reports, there’s no enforcement, and no punishment
for not filing.
It is also important to note that no one is paid to enter
this data. That could be a part time job for most clinicians, were they to
responsibly report all the side effects and deaths.
COVID Shots Are Far Deadlier Than the Infection
Overall, his team’s calculations suggest we’re killing
411 people per million doses (and remember Moderna and Pfizer are both two-dose
regimens), worldwide. And that’s just the short-term mortality. We still have
no concept of how these shots might impact mortality in the longer term.
To put things into further perspective, October 21, 2021,
an Italian investigation found that by changing the COVID mortality definition
to only include cases where COVID-19 was the primary cause of death and there
were no comorbidities decreased the death toll by 97%, from 130,000 to fewer
than 4,000.
Kirsch believes the real death tally from COVID-19 in the
U.S. may be about 50% of the reported number. This means about 380,000
Americans died from COVID-19 (rather than with COVID), whereas the COVID
“vaccine” has killed as many as 300,000. In other words, it’s possible that the
cure may be worse than the disease.
COVID Shot Is the Deadliest ‘Vaccine’ Ever Created
It gets even worse though. In Pfizer’s children’s trial,
one of the participants, 12-year-old Maddie De Garay, suffered a number of
devastating events, including paralysis. This side effect was misreported,
however, and put down as “abdominal pain.” Neither the FDA nor the CDC has
investigated the case, despite promising to do so. Pfizer has refused to
investigate it as well.
These COVID vaccines are over 800 times deadlier than the
deadliest vaccine in human history. So, this isn't a close call. These vaccines
are the deadliest vaccines ever created by man. And they're promoted as safe
and effective. ~ Steve Kirsch
In the youth trial, 1 out of 1,131 children was
paralyzed. Meanwhile, Pfizer’s adult trial shows that the shot saves one COVID
death for every 22,000 fully-vaccinated people. But for children, it’s
estimated we need to fully vaccinate over 630,000 kids to save one life. That
means we may permanently disable as many as 557 kids per life saved. Meanwhile,
there’s not a single report of a healthy child dying from SARS-CoV-2 infection
anywhere in the world.
This means the number needed to vaccinate to save one
otherwise healthy child from COVID death is actually infinite, as they’re not
dying from COVID to begin with. There simply is no doubt that in children, the
COVID shot is no benefit and all risk. Kirsch notes:
“Dr. Paul Offit was
interviewed 20 years ago on ‘CBS 60 Minutes,’ and he said the smallpox vaccine
is so dangerous that we would never consider doing that in modern times. It's
the most dangerous vaccine ever invented ... and the smallpox vaccines only
kills one person per every million-people vaccinated, which is a lot.
You vaccinate 300 million
people, you're going to kill 300 people. That is unacceptable according to
Offit, but he just voted for a vaccine that kills 822 people per million fully
vaccinated [assuming a two-dose regimen].
That means these COVID
vaccines are over 800 times deadlier than the deadliest vaccine in human
history. So, this isn't a close call. These vaccines are the deadliest vaccines
ever created by man. And they're promoted as safe and effective.”
COVID Shot Gets Deadlier the Younger You Are
Based on a request from Dr. Peter McCullough, Kirsch also
analyzed COVID jab mortality based on age using the VAERS data. For
80-year-olds, he found we kill two people to save one. For 20-year-olds, we
kill six to save one.
The younger you are, the greater the risk. The Kostoff
analysis4 found this general pattern as well.
Ronald N. Kostoff is a research affiliate in Gainesville, Virginia, who in 2016
wrote an expert review on under-reporting of adverse events in the biomedical
literature.5
In a review published in October 2021, Kostoff found five
elderly are killed by the shots for each elderly person saved, and the ratios
get worse as you go down in age. That said, “the vaccines don't make sense for
any age group, which is exactly the same thing I found independently,” Kirsch
says.
“Nobody should get these
vaccines. There is no cost-benefit analysis that I have seen that shows it is
beneficial ... I mean, you're not going to take an intervention that is just as
likely to kill you as to save you.
You want to take an
intervention which is at least 10 times more likely to save you than to kill
you, because it's an optional intervention. What kind of business do you have
taking an intervention which has a marginal benefit for a completely unknown
short- and long-term risk profile?
The other thing I want to say
is that, the societal benefit argument, people are saying, ‘You're selfish
because you didn't get vaccinated.’ Well, that's irrational.
Have you ever seen a CDC
analysis showing you the societal benefit of being vaccinated? It doesn't
exist. And there's a reason it doesn't exist, because the societal benefit
would be so tiny that it’s ludicrous. Today, we know the vaccinated are as
likely to spread the virus as the unvaccinated. So where is the societal
benefit?
If there are no downsides [to
the shot], then people would say, sure, maybe there's some societal benefit.
I'll do that. But here your life is at stake and the data show that roughly 1
in 1,000 will get killed by these vaccines. So, if I say, hey, suppose
sacrificing your life could save 100 person years (e.g., 10 people given
another 10 years of life).
When I asked this live in a
clubhouse room with a few hundred people, nobody raised their hand to volunteer
to do that — to sacrifice their life to save 100 person years. And I said, ‘OK,
what about 1,000 person years? If you could sacrifice your life to save people
1,000 person years, would you do it? Nobody would do that. It's nonsensical.
We have a constitutional right
to life ... And I don't think you're being selfish about it. You have a family,
you have friends, you have loved ones, you have people you interact with ...
Why would I ask you to sacrifice your life? To save people you don’t know?
Everybody has their own
special way that they contribute to society. Why would we ever ask somebody to
[sacrifice their life for a potential social benefit]? Maybe we should ask Joe
Biden, ‘Joe, if you could give up your life to save 1,000 person-years, would
you do that?’ It would be very interesting to see what he says.”
CDC Performs Statistical Magic, Again
Countering all of this data we have a recent CDC analysis,6
which concluded that people who get the COVID shot are two-thirds less likely
to die of any cause.
“I sent Janet Woodcock my deck
of 180 questions. I said, ‘Janet, I bet you can't answer any of these 180
questions. Doesn't this concern you?’ She sends back an email saying, ‘Look at
the CDC analysis, showing that after you get the jab, there's this two-thirds
drop in mortality.’
My friends and I, when we saw
in that paper, we were laughing our heads off over here. The stats on 18- to
44-year-olds [show] 35% die from accidents. The rest die from disease — cancer,
heart disease, whatever.
The only way to get a
two-thirds reduction [in all-cause mortality] is if nobody dies from anything
anymore — any disease — and we also reduce the number of accidents that they
have ... This is the immortality drug. All kidding aside, there's no mechanism of
action that could possibly justify that people are going to be better off from
a health perspective after getting these vaccinations. Zero.
Nothing is improved. You are
not immortal. You are just the opposite; your immune system is compromised.
You're also more likely to get COVID. In the U.K., the government numbers show
that 40-year-olds, after the honeymoon period is over, were more than twice as
likely to get infected if they were vaccinated.
In the U.S., you have
hospitals where you have a 50% community vaccination rate and the hospital
admissions are 90% vaccinated people. You can't make these statistics up.
In fact, the CDC was
confronted by these statistics by Aaron Siri, who wrote about it on his
substack, and they just ignored them. So, they make up stuff [and] this paper
shows the CDC can put out anything and as long as it has that little CDC logo
on it, people are going to believe it no matter how ridiculous it is.
And nobody in the medical
community criticized it. I wrote a very popular article about it on my substack
entitled, ‘FDA Discovers Fountain of Youth.’”
Biggest Fraud in History
All things considered, the COVID vaccination campaign is
the biggest medical fraud in modern history. As Kirsch says, it’s a house of
cards, held together by belief in data that aren’t there and avoidance of
confronting the safety signals in the VAERS system and other studies that don’t
comport with the narrative.
They even avoided the determination of one of the world’s
top pathologists (Peter Schirmacher) that at least 30% to 40% of the deaths two
weeks post-vaccine were caused by the vaccine. The still claim there are no
deaths that have been attributed to the Pfizer or Moderna vaccines. That’s
ridiculous.
“I've never seen anything like
this, and I've never heard of anything like this because the conspirators who
are telling this false narrative are all the three-letter agencies under the
Department of Health and Human Services — the FDA, CDC and NIH.
They're all in on it, Congress
is all in on it, mainstream media's all in on it, and the medical community is
all in on it. They can’t afford to back down now because they are in it too
deep. It would be too embarrassing to them.
We have been saying for
months, ‘You guys have to look at the VAERS data,’ and they have been ignoring
and censoring us rather than engaging us with dialogue — and none of these
people will engage us in dialogue.
We tell the so-called ‘fact
checkers’ where to look and what questions to ask the CDC to verify our stories
and they never follow up. The ‘fact checkers’ all refuse to get on a recorded
phone or Zoom call since they don’t want to be exposed as being biased.
One strategy for changing this
is that we're going to run a series of ads. Each of the ads will feature a
unique personality, like a Dr. Peter McCullough, a sports figure, doctors,
victims and so on. They'll relate their personal anecdotes for what's happened
to them. And they will say, ‘Look, before you get vaccinated, check the facts.
Listen to the other side of the story.’
It's a reasonable ask. And
we’ll direct them where to go to hear the side of the story that the mainstream
media aren’t allowing them to hear. And then we let them make up their own
mind. People aren't hearing the other side of the story, and the White House is
helping suppress it. When the White House has a hit list of censorship, it's
very clear what is going on. When in history have we done that?
Do you ever see McCullough on
CNN? No, because they want to give you only one side and they're deliberately
giving you only one side of it, and they know it. If they want to give the
impression they are balanced, they’ll pick someone who isn’t an expert and
interview them. Robert Malone is never going to be on CNN. Malone invented the
mRNA vaccine and yet he doesn’t qualify to talk about it on CNN?
America used to be a country
that embraced a diversity of views, and you had freedom of speech, you had
freedom to express your opinion. You had the freedom to tell the truth. No
more. That freedom has been taken away.
If you don't agree with the
mainstream narrative, you're silenced. And so, what we're going to do is run
the series of ads, and we'll only be able to run it on alternate media because
the mainstream media won't run our ads because the ads encourage people to hear
the other side of the issue.”
More Information
Again, you can download Kirsch’s 177-page
PDF,
jam-packed with questions and data on the COVID “vaccine.” I also urge you to
review his “False Narrative Takedown” (TFNT) series, which you can find on his Rumble channel.
You can also peruse his website, skirsch.io, or
follow him on his social media accounts, which include Twitter, Gab, Telegram and
LinkedIn. To
keep on top of his latest investigations, you can subscribe to his Substack
channel. If you can afford it, consider signing up for a paid
subscription. Select articles can also be found on TrialSiteNews.
“Substack is really important
because they don’t censor people who tell the truth,”
Kirsch says. “So, I really encourage
people to support platforms like Substack. I also get a portion of that, and
any money I get, I will donate 100% to funding ads and to fighting this. If we
can get 100,000 subscribers at $5 a month, that's $500,000 a month we can spend
to combat false narrative. That's serious fire power.
People ask me, why am I doing
this? I'm not making any money off of this. I have no conflicts of interest. I
have no history as a conspiracy theorist or spreader of misinformation. We’ve
lost all our friends. I
was forced out of my job because I wanted to speak out against the vaccines.
I'm losing money on this
because I'm funding a lot of the things out of my personal pocketbook. The
donors that donated to the early treatment fund, none of them, not a single
one, is supporting the effort to get the truth out about how dangerous these
vaccines are and how wrong the mandates are.
My motivation is a 100% on
saving lives. That's my reward in life. If I can save one life, my life was
worth living. If I can save 100 lives, even better. If I can save 100,000
lives, that is more meaningful than anything I’ve ever done or will do.”
Sources and
References
- 1 The Expose September 18, 2021
- 2 Questions
about the COVID vaccine (PDF)
- 3 SKirsch.io/vaccine-resources
- 4 Toxicology Reports September 2021; 8: 1665-1684
- 5 Journal
of Data and Information Science Vol 1, No. 4. 2016
- 6 CDC MMWR October 29, 2021; 70(43): 1520-1524
===========
m.
Story
#1: UN-Backed Banker Alliance Announces “Green” Plan
to
Transform the Global Financial System
https://www.corbettreport.com/nwnw20211111/?utm_source=feedburner&utm_medium=email
with James Corbett and James Evens Pilato
(28:31)
+
COP26: Black Agenda Report Special
Issue
http://www.blackagendareport.com/cop26-black-agenda-report-special-issue
with
António Guterres, UN Secretary General
(6:55)
+
COP-26: UN SG Blasts Climate Agreement
http://www.informationclearinghouse.info/56860.htm
by
+
Industrial Nations Value Capitalism Over People at Global
Climate Conference
by Anthony
Karefa Rogers-Wright
+
Using the Climate Crisis: Whitney Webb Discusses Global Elites’
Takeover of Nature
by
+
Behind the Scenes at COP26: Developing Countries Fume Over
U.S. Pressure to Alter Climate Finance Terms
by Rishika
Pardikar
+
COP26 Was a Failure But the People's Alternative
Can Still Be a Success
http://www.blackagendareport.com/cop26-was-failure-peoples-alternative-can-still-be-success
+
Climate Lockdowns Begin, "Fully Vaccinated"
Now Defined As 3 Shots & OSHA Suspends Biden Jab Mandate
with Ryan
Cristián
(2:14:40)
+
The
Fiscal-Military-Corporate State We Cannot Sustain
https://www.counterpunch.org/2021/11/18/the-fiscal-military-corporate-state-we-cannot-sustain/
by Mark Muhich
===========
n.
Big Pharma, GOP Plot to Use Senate Parliamentarian
to Stop Drug Price Reforms
by Jake
Johnson
+
"Patients
at Sentara Norfolk General Hospital are Dying Needlessly."
https://covid19criticalcare.com/
by Dr. Paul Marik
+
Massive
COVID Surge Rattles Europe,
Putting
US at Risk Ahead of Thanksgiving
by William Rivers Pitt
+
Hiring a diverse police force may change what cops look like,
but it doesn't change what policing
means and does

by Reina
Sultan
+
We can decide that we won’t live and
die on these terms
with Kelly Hayes
(audio, 17:42)
===========
o.
Why Are Moderna’s Billionaires
Airbrushing Scientists
Out of the Vaccine Patent Picture?
by Sam
Pizzigati
+
The Marine Corps won’t expel all
unvaccinated Marines en masse
on the Nov. 28 deadline, Navy secretary
says
https://taskandpurpose.com/news/marine-corps-navy-secretary-covid-vaccine-mandate/
by Jeff
Schogol
+
20 Years After Patriot Act,
Surveillance of Arabs and Muslims Is Relentless
by Nadine
Naber
+
60 US Health Groups Urge Companies
to Voluntarily Implement Blocked
Vaccine Rule

by Kenny
Stancil
===========
p.
Pegasus is Just the Tip of the Israeli
Cyber Spying Iceberg
https://www.mintpressnews.com/pegasus-just-tip-israel-unit-8200-toka-spyware-whitney-webb/278042/
with Whitney Webb and Mnar Adley
(49:49)
+
Did Israel's May attack cause
miscarriages?
https://electronicintifada.net/content/did-israels-may-attack-cause-miscarriages/34311
by Sarah
Algherbawi
+
Miss South Africa shamed for refusing
to boycott Israel
https://electronicintifada.net/blogs/tamara-nassar/miss-south-africa-shamed-refusing-boycott-israel
by Tamara
Nassar
+
Exposing Israel's Use of Settler
Aggression to Grab Palestinian Land
https://www.globalresearch.ca/exposing-israel-use-settler-aggression-grab-palestinian-land/5762028
by Michael
Jansen
+
Meet Blackstone Israel's secret weapon
https://www.jpost.com/50-most-influential-jews/yifat-oron-678150
by Zev Stub
===========
q.
Democratic accountability keeps
revolutions alive
https://therealnews.com/democratic-accountability-keeps-revolutions-alive
with Marc
Steiner and Circles Robinson
(audio,
29:13)
+
Even in solidly blue states, Democrats aren’t pursuing
serious progressive change
by Luke Savage
+
Operation Coronavirus:
How the Masses Were Hypnotized into the
COVID Cult
https://www.globalresearch.ca/how-masses-hypnotized-covid-cult/5762017
by Makia
Freeman
+
Censorship is the Last Gasp of the
Liberal Class
http://www.blackagendareport.com/censorship-last-gasp-liberal-class
by Danny
Haiphong
+
Adam
Schiff And The End Of Shame In American Politics
https://www.zerohedge.com/political/adam-schiff-and-end-shame-american-politics
by Jonathan
Turley
===========
r.
Australian War Propaganda Keeps Getting
Crazier
http://www.informationclearinghouse.info/56864.htm
by Caitlin Johnstone
+
New files expose Australian govt’s betrayal of Julian Assange
and
detail his prison torment
https://thegrayzone.com/2021/11/17/files-australian-julian-assange-prison/
by Kit Klarenberg
+
Former
prime minister Paul Keatin addresses the National Press Club
http://www.informationclearinghouse.info/56858.htm
with former Australian prime minister Paul Keatin
(1:17:45)
+
The managed destruction of Australia’s
oldest faculty of Arts
https://overland.org.au/2021/11/the-managed-destruction-of-australias-oldest-faculty-of-arts/
by Nick Riemer
===========
s.
“Welcome to the New Economy”

https://www.corbettreport.com/welcome-to-the-new-economy/
with James
Corbett
+
Davos Billionaires Want to Save the Planet…
‘The Repackaging of Eugenics’
by Matthew
Ehret-Kump
+
Leases for more oil drilling are flying to anyone who can write the U.S.
government a big enough check
by William
Rivers Pitt
+
9/11 and the Politics of Fear and
Self-Preservation
with Whitney
Webb
(2:21:07)
===========
t.
Kellogg’s
strikers hold the line and prepare for winter
https://therealnews.com/kelloggs-strikers-hold-the-line-and-prepare-for-winter
by Mel Buer
+
Two
climate activists halt operations at world's largest coal port
https://therealnews.com/two-climate-activists-halt-operations-at-worlds-largest-coal-port
by Julia Conley
+
Baltimore
museum workers are fighting for a 'wall-to-wall' union
https://therealnews.com/baltimore-museum-workers-are-fighting-for-a-wall-to-wall-union
with Maximillian Alvarez, Laura Albans, and Matt Papich
(41:48)
===========
u.
Outcome
Reporting Bias in COVID-19 mRNA Vaccine Clinical
https://www.oyetimes.com/wp-content/uploads/2021/05/medicina-57-00199.pdf
by Ronald B. Brown
+
Why Is The Media Suddenly No Longer Interested In Blaming
COVID Waves On Red States
by ‘IM' via 'Unmasked'
Substack
+
Access to Information Is the Key to
Truth
https://www.globalresearch.ca/global-research-access-information-key-truth/5746757
+
How
to Find Deleted Videos
https://www.corbettreport.com/qfc081-deletedvideos/?utm_source=feedburner&utm_medium=email
with James Corbett
(9:26)
===========
v.
Locking
Down Unvaccinated-Only ‘Not About Science,
It’s
About Punishing People’

by Jeremy Loffredo
+
Vidéos of growing protests against the vaccine
that are censored in the corporate
media
https://www.bitchute.com/video/NvI4Er74uIqq/
+
Days Into Lockdown For The Unvaccinated,
Austria
COVID Cases Hit Record High

https://www.zerohedge.com/covid-19/days-lockdown-unvaccinated-austria-covid-cases-hit-record-high
by Tyler Durden
+
Austrian cops and military joining the resistance
to Big Pharma’s
Anschluss
by Mark Crispin Miller
+
Germany Preparing To Impose Austria-Style
Lockdown On The Unvaxx'd

https://www.zerohedge.com/covid-19/germany-preparing-impose-austria-style-lockdown-unvaxxd
by Paul
Joseph Watson via Summit News
+
Frozen Deutschland
http://www.informationclearinghouse.info/56866.htm
by Pepe Escobar
+
Italian
Governors Call For Unvaccinated To Be Put Under Lockdown
https://www.zerohedge.com/covid-19/italian-governors-call-unvaccinated-be-put-under-lockdown
by Paul
Joseph Watson via Summit News
+
93%-Vaccinated
Ireland Has Gone Back Into 'Partial Lockdown',
Including
Midnight Curfew
by Tyler Durden
+
Myth vs. Reality in COVID Russia


https://www.globalresearch.ca/myth-vs-reality-covid-russia/5762059
by Riley Waggaman
+
NATO
Increases Military Flights Along Belarus Border
As Putin Blames EU For Migrant Crisis

by Tyler Durden
+
G7 Nations Issue Scathing Condemnation Of Belarus
Using

by Tyler Durden
===========
w.
The nature of neoliberalism and its
consequences
with Chris
Hedges
(25:19)
+
‘I Wish We Had A Real Border Czar’:
Texas
Dem Congressman Slams VP Kamala Harris
by Tyler Durden
+
Over $53 Million In Meth, Coke, & Pot Seized By Border Patrol
In Texas
https://www.zerohedge.com/markets/over-53-million-meth-coke-and-pot-seized-border-patrol-texas
by Truckers
News Staff
+
Will
You Storm the Capitol if the 2024 Election is Stolen?
https://www.counterpunch.org/2021/11/18/will-you-storm-the-capitol-if-the-2024-election-is-stolen/
by Thom Hartmann
===========
x.
The Tripartite World Order and the
Hybrid World War
http://www.informationclearinghouse.info/56869.htm
by Dmitry Orlov
+
How
The "Grand Chessboard" Led To US Checkmate In Afghanistan

https://www.zerohedge.com/geopolitical/how-grand-chessboard-led-us-checkmate-afghanistan
by Max
Parry via Off-Guardian.org,
+
U.S.
Terrorism 101: The Bert Sacks Story
http://www.informationclearinghouse.info/56868.htm
by Edward Curtin
+
How the U.S. Lost the "Great Game" in Central Asia

https://covertactionmagazine.com/2021/11/08/how-the-u-s-lost-the-great-game-in-central-asia/
by Aidan O’Brien
+
Syria's My Lai? US massacred 70
civilians and covered it up

http://www.informationclearinghouse.info/56861.htm
by Aaron Maté
===========
y.
Organizing Against Racism and Class
Oppression
http://www.blackagendareport.com/organizing-against-racism-and-class-oppression
by Danny
Haiphong
+
Don’t black lives matter if those
“vaccines” take them?
https://markcrispinmiller.com/2021/08/dont-black-lives-matter-if-those-vaccines-take-them/
by Mark Crispin Miller
+
F.W. de Klerk: Requiem for a Racist Murderer
http://www.blackagendareport.com/fw-de-klerk-requiem-racist-murderer
by Dr. Marsha Coleman-Adebayo
===========
z.
Let a Hundred Socialist Flowers Bloom:
A Conversation with Issa Shivji
http://www.blackagendareport.com/let-hundred-socialist-flowers-bloom-conversation-issa-shivji
by Issa
Shivji
+
Glen Ford: In Memoriam
http://www.blackagendareport.com/glen-ford-memoriam
by Peter
James Hudson and Jemima Pierre
+
Vietnamese National Hero, Colonel
Đặng Văn Việt,
Who Helped Vietnam End Its Colonial
Scourge,
Dies at Age 102

by Felix Abt
+
Sent: Monday, November 22, 2021
Subject: [H-PAD] H-PAD Notes 11/22/21: Panels on "Twenty Years of War"; Links to recent articles of interest
Note: Historian Tejasvi Nagaraja at Cornell University will host two free online panels under the theme of "Twenty Years of War." The first, "The War on Terror, Security Statecraft, and Racial Justice," takes place November 30 and the second, "Coalitions of War and Antiwar," on December 7, both at 3pm EST.
Links to Recent Articles of Interest
"To Govern the Globe: Washington's World Order and Catastrophic Climate Change
By Alfred McCoy, TomDispatch.com, posted November 18
Based on the author's new book, To Govern the Globe (Dispatch Books, November 2021), which covers the last 600 years of "world orders" and their unmaking, this article argues that climate change is eclipsing America's world order and offering only a short duration for the China-dominated order that is likely to follow. The author teaches history at the University of Wisconsin.
"Are We Witnessing a 'General Strike' in Our Own Time?"
By Nelson Lichtenstein, Washington Post, posted November 18
Compares the current phenomenon of workers leaving their jobs, sometimes called "The Great Resignation," with W. E. B. Du Bois's use of the term "general strike" for actions by African Americans' in the South during and after the Civil War. The author is a labor historian and a research professor at the University of California, Santa Barbara.
"As One of the First White Kids in a Black School, I Learned Not to Fear History"
By Woody Holton, Washington Post, posted November 12
A personal account by University of South Carolina historian Woody Holton, who attended a newly integrated public school in Richmond in the early 1970s. His father, Linwood Holton, was the Republican governor of Virginia at the time and accepted federal court orders to desegregate the schools. The older Holton died on October 28 of this year.
"The 1619 Project and the Long Battle over U.S. History"
By Jake Silverstein, New York Times, posted November 9
"Fights over how we tell our national story go back more than a century — and have a great deal to teach us about our current divisions." The author is the editor-in-chief of the New York Times Magazine and a key figure in the 1619 Project.
"Educational Gag Orders: Legislative Restrictions on the Freedom to Read, Learn, and Teach."
A report by PEN America, posted November 8
A detailed survey of the 54 bills introduced in 24 state legislatures during January-September 2021 to restrict teaching and training in K-12 schools, public universities, and state agencies. "These bills appear designed to chill academic and educational discussions and impose government dictates on teaching and learning. In short: They are educational gag orders."
"The CIA Undermined Postcolonial Africa from the Start"
By Alex Park, Jacobin, posted November 7
A review essay on Susan Williams's book White Malice: The CIA and the Recolonization of Africa (Public Affairs Press, 2021), a deeply researched account of how the CIA undermined leftist governments in the Congo and Ghana in the late 1950s and early 1960s. The reviewer is a freelance journalist with a particular interest in foreign investments in Africa.
"White Backlash Is America's Most Destructive Habit"
By John S. Huntington and Lawrence B. Glickman, The Atlantic, posted November 7
Gives historical examples, starting with Reconstruction, showing that "Each time political minorities advocate for and achieve greater equality, conservatives rebel, trying to force a reinstatement of the status quo." The authors teach history at Houston Community College and Cornell University, respectively.
"Armaud Arbery Suspects' Trial Defense Taps a Racist Legal Legacy"
By Alan Singer, Think, posted November 5
"The idea of citizen’s arrest laws dates to Europe in the 13th century, but it became melded with American efforts to prevent slave escapes." The author is a historian and director of social studies education at Hofstra University.
"Loose Talk"
By Steven Shapin, London Review of Books, posted November 4
A lengthy review-essay on Alex Wellerstein's book Restricted Data: The History of Nuclear Secrecy in the United States (U. of Chicago Press, 2021). The reviewer is a professor emeritus of the history of science at Harvard University.
"The Historians Are Fighting"
By William Hogeland, Slate, posted October 30
An informative and entertaining account of the recent face-off at the Massachusetts Historical Society between Woody Holton and Gordon Wood on the 1619 Project and the nature of the American Revolution. The author has published several books on early American history, including Inventing America (MIT Press, 2009).
Thanks to an anonymous reader for flagging some of the articles included above, and to Steve Gosch for valuable consultation. Suggestions can be sent to jimobrien48@gmail.com.